Rahardjo Theresia Monica, Maskoen Tinni Trihartini, Redjeki Ike Sri
Anesthesiology Department, Faculty of Medicine, Maranatha Christian University, Bandung, Indonesia.
Anesthesiology & Intensive Care Department, Faculty of Medicine, Universitas Padjadjaran, Bandung, Indonesia.
J Med Case Rep. 2016 Aug 26;10(1):238. doi: 10.1186/s13256-016-1034-0.
Recovery from cytomegalovirus meningoencephalitis with brain stem death in an immunocompetent patient is almost impossible. We present a remarkable recovery from a possible cytomegalovirus infection in an immunocompetent man who had severe neurological syndromes, suggesting brain stem death complicated by pneumonia and pleural effusion.
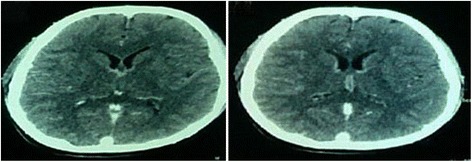
A 19-year-old Asian man presented at our hospital's emergency department with reduced consciousness and seizures following high fever, headache, confusion, and vomitus within a week before arrival. He was intubated and sent to our intensive care unit. He had nuchal rigidity and tetraparesis with accentuated tendon reflexes. Electroencephalography findings suggested an acute structural lesion at his right temporal area or an epileptic state. A cerebral spinal fluid examination suggested viral infection. A computed tomography scan was normal at the early stage of disease. Immunoglobulin M, immunoglobulin G anti-herpes simplex virus, and immunoglobulin M anti-cytomegalovirus were negative. However, immunoglobulin G anti-cytomegalovirus was positive, which supported a diagnosis of cytomegalovirus meningoencephalitis. His clinical condition deteriorated, spontaneous respiration disappeared, cranial reflexes became negative, and brain stem death was suspected. Therapy included antivirals, corticosteroids, antibiotics, anticonvulsant, antipyretics, antifungal agents, and a vasopressor to maintain hemodynamic stability. After 1 month, he showed a vague response to painful stimuli at his supraorbital nerve and respiration started to appear the following week. After pneumonia and pleural effusion were resolved, he was weaned from the ventilator and moved from the intensive care unit on day 90.
This case highlights several important issues that should be considered. First, the diagnosis of brain stem death must be confirmed with caution even if there are negative results of brain stem death test for a long period. Second, cytomegalovirus meningoencephalitis should be considered in the differential diagnosis even for an immunocompetent adult. Third, accurate therapy and simultaneous intensive care have very important roles in the recovery process of patients with cytomegalovirus meningoencephalitis.
免疫功能正常的患者若发生伴有脑干死亡的巨细胞病毒性脑膜脑炎,几乎不可能康复。我们报告了一名免疫功能正常的男性,他患有严重的神经综合征,疑似由巨细胞病毒感染所致,最初提示脑干死亡并伴有肺炎和胸腔积液,但最终实现了显著康复。
一名19岁的亚洲男性因在入院前一周内出现高热、头痛、意识模糊和呕吐后意识减退及癫痫发作,就诊于我院急诊科。他被插管并送入重症监护病房。他有颈项强直和四肢轻瘫,腱反射亢进。脑电图检查结果提示右侧颞叶区域有急性结构性病变或癫痫状态。脑脊液检查提示病毒感染。疾病早期计算机断层扫描结果正常。抗单纯疱疹病毒免疫球蛋白M、免疫球蛋白G及抗巨细胞病毒免疫球蛋白M均为阴性。然而,抗巨细胞病毒免疫球蛋白G呈阳性,这支持了巨细胞病毒性脑膜脑炎的诊断。他的临床状况恶化,自主呼吸消失,颅神经反射呈阴性,疑似脑干死亡。治疗包括抗病毒药物、皮质类固醇、抗生素、抗惊厥药、退烧药、抗真菌药以及一种血管升压药以维持血流动力学稳定。1个月后,他对眶上神经的疼痛刺激有模糊反应,第二周开始出现呼吸。肺炎和胸腔积液消退后,他于第90天脱机并转出重症监护病房。
该病例突出了几个应予以考虑的重要问题。首先,即使脑干死亡测试长期呈阴性结果,也必须谨慎确认脑干死亡的诊断。其次,即使是免疫功能正常的成年人,在鉴别诊断时也应考虑巨细胞病毒性脑膜脑炎。第三,准确的治疗和同步的重症监护在巨细胞病毒性脑膜脑炎患者的康复过程中起着非常重要的作用。