van den Hof Susan, Collins David, Hafidz Firdaus, Beyene Demissew, Tursynbayeva Aigul, Tiemersma Edine
KNCV Tuberculosis Foundation, The Hague, The Netherlands.
Amsterdam Institute for Global Health and Development and Academic Medical Center, Amsterdam, The Netherlands.
BMC Infect Dis. 2016 Sep 5;16(1):470. doi: 10.1186/s12879-016-1802-x.
One of the main goals of the post-2015 global tuberculosis (TB) strategy is that no families affected by TB face catastrophic costs. We revised an existing TB patient cost measurement tool to specifically also measure multi-drug resistant (MDR) TB patients' costs and applied it in Ethiopia, Indonesia and Kazakhstan.
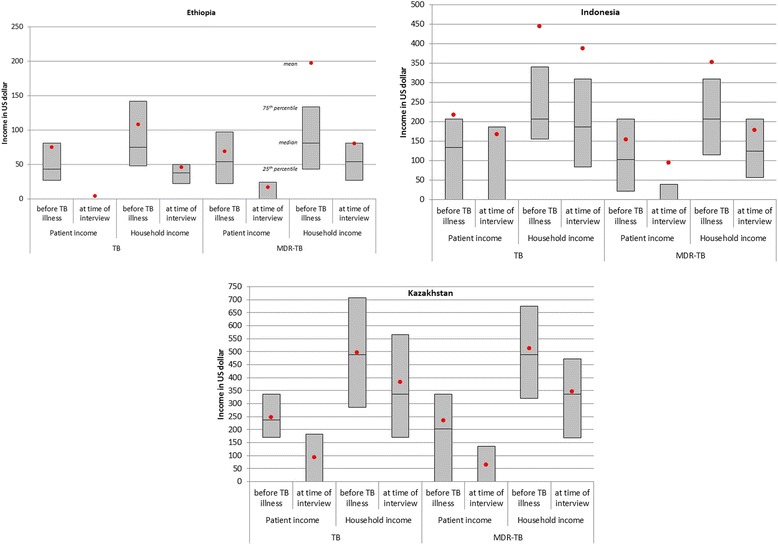
Through structured interviews with TB and MDR-TB patients in different stages of treatment, we collected data on the direct (out of pocket) and indirect (loss of income) costs of patients and their families related to the diagnosis and treatment of TB and MDR-TB. Direct costs included costs for hospitalization, follow-up tests, transport costs for health care visits, and food supplements. Calculation of indirect costs was based on time needed for diagnosis and treatment. Costs were extrapolated over the patient's total treatment phase.
In total 406 MDR-TB patients and 197 other TB patients were included in the survey: 169 MDR-TB patients and 25 other TB patients in Ethiopia; 143 MDR-TB patients and 118 TB patients in Indonesia; and 94 MDR-TB patients and 54 other TB patients in Kazakhstan. Total costs for diagnosis and current treatment episode for TB patients were estimated to be USD 260 in Ethiopia, USD 169 in Indonesia, and USD 929 in Kazakhstan, compared to USD 1838, USD 2342, and USD 3125 for MDR-TB patients, respectively. These costs represented 0.82-4.6 months of pre-treatment household income for TB patients and 9.3-24.9 months for MDR-TB patients. Importantly, 38-92 % reported income loss and 26-76 % of TB patients lost their jobs due to (MDR) TB illness, further aggravating the financial burden.
The financial burden of MDR-TB is alarming, although all TB patients experienced substantial socioeconomic impact of the disease. If the patient is the breadwinner of the family, the combination of lost income and extra costs is generally catastrophic. Therefore, it should be a priority of the government to relieve the financial burden based on the cost mitigation options identified.
2015年后全球结核病(TB)战略的主要目标之一是确保没有受结核病影响的家庭面临灾难性费用。我们修订了现有的结核病患者成本测量工具,以专门测量耐多药(MDR)结核病患者的成本,并在埃塞俄比亚、印度尼西亚和哈萨克斯坦应用了该工具。
通过对处于不同治疗阶段的结核病和耐多药结核病患者进行结构化访谈,我们收集了患者及其家庭与结核病和耐多药结核病诊断及治疗相关的直接(自付)和间接(收入损失)成本数据。直接成本包括住院费用、随访检查费用、就医交通费用和营养补充剂费用。间接成本的计算基于诊断和治疗所需的时间。成本推算涵盖患者的整个治疗阶段。
该调查共纳入406例耐多药结核病患者和197例其他结核病患者:埃塞俄比亚有169例耐多药结核病患者和25例其他结核病患者;印度尼西亚有143例耐多药结核病患者和118例结核病患者;哈萨克斯坦有94例耐多药结核病患者和54例其他结核病患者。结核病患者诊断和当前治疗阶段的总成本估计在埃塞俄比亚为260美元,在印度尼西亚为169美元,在哈萨克斯坦为929美元,而耐多药结核病患者分别为1838美元、2342美元和3125美元。这些成本分别占结核病患者治疗前家庭收入的0.82 - 4.6个月和耐多药结核病患者的9.3 - 24.9个月。重要的是,38% - 92%的患者报告有收入损失,26% - 76%的结核病患者因(耐多药)结核病而失业,这进一步加重了经济负担。
耐多药结核病的经济负担令人担忧,尽管所有结核病患者都经历了该疾病对社会经济的重大影响。如果患者是家庭的主要经济支柱,收入损失和额外费用相结合通常具有灾难性。因此,政府应根据确定的成本减轻方案,将减轻经济负担作为优先事项。