Mazarova Andrea, Molnar Amber O, Akbari Ayub, Sood Manish M, Hiremath Swapnil, Burns Kevin D, Ramsay Timothy O, Mallick Ranjeeta, Knoll Gregory A, Ruzicka Marcel
Division of Nephrology, Department of Medicine, The Ottawa Hospital, Ottawa, Canada.
Division of Nephrology, Department of Medicine, McMaster University, Hamilton, Canada.
BMC Nephrol. 2016 Sep 5;17(1):123. doi: 10.1186/s12882-016-0338-z.
Restriction of dietary sodium is routinely recommended for patients with chronic kidney disease (CKD). Whether or not sodium intake is associated with the progression of CKD and mortality remains controversial. We evaluated the association of urinary sodium excretion (as a surrogate for sodium intake) on the need for renal replacement therapy and mortality in patients with advanced CKD.
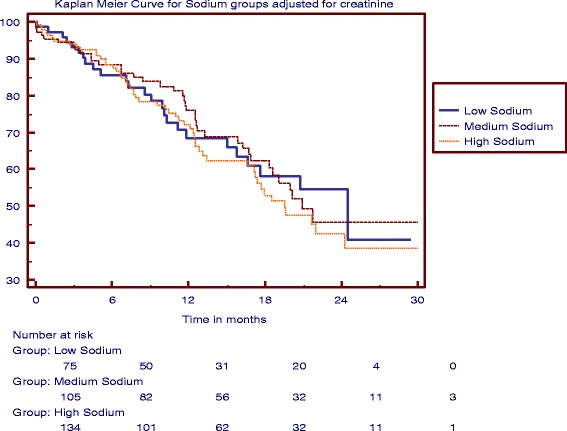
We conducted a retrospective study of patients followed at a CKD clinic of a tertiary care hospital from January 2010 to December 2012. Adult patients with advanced CKD (estimated glomerular filtration rate (eGFR) <30 ml/min/1.73 m(2)) were included. Using a time-to-event analysis, we examined the association of urinary sodium excretion as a continuous and also as a categorical variable (categorized as low sodium diet - LSD (<100 mEq/day), medium sodium diet - MSD (100-150 mEq/day), and high sodium diet - HSD (>150 mEq/day) and the outcomes of interest. The primary outcome was defined as composite of progression to end-stage renal disease requiring any type of renal replacement therapy and mortality. The secondary outcome was change in eGFR/year.
341 patients (82 LSD, 116 MSD and 143 HSD) were included in the study (mean follow up of 1.5 years) with a mean eGFR decline of 2.7 ml/min/1.73 m(2)/year. 105 patients (31 %) required renal replacement therapy and 10 (3 %) died. There was no association between urinary sodium excretion and change in the eGFR or need for renal replacement therapy and mortality in crude or adjusted models (unadjusted HR 1.002; 95%CI 1.000-1.004, adjusted HR 1.001; 95%CI 0.998-1.004).
In patients with advanced CKD (eGFR < 30 ml/min/1.73 m(2)), sodium intake does not appear to impact the progression of CKD to end-stage renal disease; however, more definitive studies are needed.
对于慢性肾脏病(CKD)患者,常规建议限制饮食中的钠摄入。钠摄入量是否与CKD进展及死亡率相关仍存在争议。我们评估了尿钠排泄(作为钠摄入的替代指标)与晚期CKD患者肾脏替代治疗需求及死亡率之间的关联。
我们对2010年1月至2012年12月在一家三级护理医院的CKD门诊随访的患者进行了一项回顾性研究。纳入成年晚期CKD患者(估计肾小球滤过率(eGFR)<30 ml/min/1.73 m²)。采用事件发生时间分析,我们将尿钠排泄作为连续变量以及分类变量(分为低钠饮食-LSD(<100 mEq/天)、中钠饮食-MSD(100-150 mEq/天)和高钠饮食-HSD(>150 mEq/天))来检验其与感兴趣的结局之间的关联。主要结局定义为进展至需要任何类型肾脏替代治疗的终末期肾病和死亡的复合结局。次要结局为每年eGFR的变化。
341例患者(82例LSD、116例MSD和143例HSD)纳入研究(平均随访1.5年),eGFR平均每年下降2.7 ml/min/1.73 m²。105例患者(31%)需要肾脏替代治疗,10例(3%)死亡。在粗模型或校正模型中,尿钠排泄与eGFR变化、肾脏替代治疗需求及死亡率之间均无关联(未校正HR 1.002;95%CI 1.000-1.004,校正HR 1.001;95%CI 0.998-1.004)。
在晚期CKD(eGFR <30 ml/min/1.73 m²)患者中,钠摄入似乎不会影响CKD进展至终末期肾病;然而,仍需要更确切的研究。