Zwingmann J, Lefering R, Feucht M, Südkamp N P, Strohm P C, Hammer T
Department of Orthopedics and Trauma Surgery, Freiburg University Hospital, Hugstetter Str. 55, 79098, Freiburg, Germany.
Institute for Research in Operative Medicine (IFOM), University of Witten/Herdecke, Herdecke, Germany.
Crit Care. 2016 Sep 6;20(1):282. doi: 10.1186/s13054-016-1463-6.
Data of the TraumaRegister DGU® were analyzed to derive survival rates, neurological outcome and prognostic factors of patients who had suffered traumatic cardiac arrest in the early treatment phase.
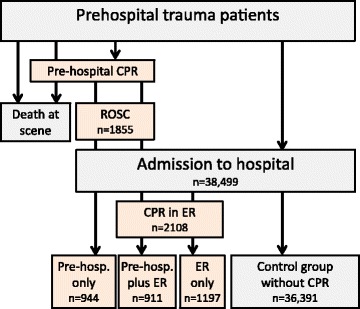
The database of the TraumaRegister DGU® from 2002 to 2013 was analyzed. The main focus of this survey was on different time points of performed resuscitation. Descriptive and multivariate analyses (logistic regression) were performed with the neurological outcome (Glasgow Outcome Scale) and survival rate as the target variable. Patients were classified according to CPR in the prehospital phase and/or in the emergency room (ER). Patients without CA served as a control group. The database does not include patients who required prehospital CPR but did not achieve ROSC.
A total of 3052 patients from a total of 38,499 cases had cardiac arrest during the early post-trauma phase and required CPR in the prehospital phase and/or in the ER. After only prehospital resuscitation (n = 944) survival rate was 31.7 %, and 14.7 % had a good/moderate outcome. If CPR was required in the ER only (n = 1197), survival rate was 25.6 %, with a good/moderate outcome in 19.2 % of cases. A total of 4.8 % in the group with preclinical and ER resuscitation survived, and just 2.7 % had a good or moderate outcome. Multivariate logistic regression analysis revealed the following prognostic factors for survival after traumatic cardiac arrest: prehospital CPR, shock, coagulopathy, thorax drainage, preclinical catecholamines, unconsciousness, and injury severity (Injury Severity Score).
With the knowledge that prehospital resuscitated patients who not reached the hospital could not be included, CPR after severe trauma seems to yield a better outcome than most studies have reported, and appears to be more justified than the current guidelines would imply. Preclinical resuscitation is associated with a higher survival rate and better neurological outcome compared with resuscitation in the ER. If resuscitation in the ER is necessary after a preclinical performed resuscitation the survival rate is marginal, even though 56 % of these patients had a good and moderate outcome. The data we present may support algorithms for resuscitation in the future.
分析创伤注册数据库DGU®的数据,以得出创伤后早期接受创伤性心脏骤停治疗患者的生存率、神经功能结局及预后因素。
分析2002年至2013年创伤注册数据库DGU®的数据。本次调查的主要重点是进行复苏的不同时间点。以神经功能结局(格拉斯哥预后评分)和生存率作为目标变量进行描述性分析和多变量分析(逻辑回归)。根据院前阶段和/或急诊室(ER)的心肺复苏情况对患者进行分类。未发生心脏骤停的患者作为对照组。该数据库不包括需要院前心肺复苏但未实现自主循环恢复的患者。
在总共38499例病例中,共有3052例患者在创伤后早期发生心脏骤停,需要院前阶段和/或急诊室进行心肺复苏。仅院前复苏(n = 944)后的生存率为31.7%,14.7%的患者结局良好/中等。若仅在急诊室需要心肺复苏(n = 1197),生存率为25.6%,19.2%的病例结局良好/中等。院前和急诊室复苏组中共有4.8%的患者存活,仅有2.7%的患者结局良好或中等。多变量逻辑回归分析揭示了创伤性心脏骤停后生存的以下预后因素:院前心肺复苏、休克、凝血功能障碍、胸腔引流、院前使用儿茶酚胺、昏迷和损伤严重程度(损伤严重度评分)。
鉴于未将未送达医院的院前复苏患者纳入研究,严重创伤后的心肺复苏似乎比大多数研究报告的结果更好,且似乎比当前指南所暗示的更合理。与急诊室复苏相比,院前复苏与更高的生存率和更好的神经功能结局相关。若在院前进行复苏后仍有必要在急诊室进行复苏,生存率很低,尽管这些患者中有56%的结局良好或中等。我们提供的数据可能会为未来的复苏算法提供支持。