Manz Kristin, Krug Susanne, Schienkiewitz Anja, Finger Jonas David
Department of Epidemiology and Health Monitoring, Robert Koch-Institute, PO Box 650261, 13302, Berlin, Germany.
BMC Public Health. 2016 Sep 6;16(1):939. doi: 10.1186/s12889-016-3615-7.
Organised sports (OS) participation is an important health behaviour but it seems to decline from childhood to adolescence. The aim of this study was to investigate OS participation patterns from childhood to adolescence and potential determinants for those patterns.
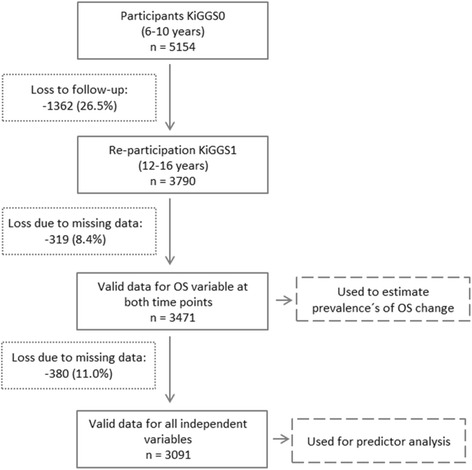
Data from the German Health Interview and Examination Survey for Children and Adolescents (KiGGS) cohort study with a 6 year follow-up period were used (KiGGS0: 2003-06, KiGGS1: 2009-12). Participants aged 6-10 years at KiGGS0, who were aged 12-16 at KiGGS1, were included (n = 3790). The outcome variable was 'OS participation' between KiGGS0 and KiGGS1 with the categories 'maintenance' (reference), 'dropout', 'commencement' and 'nonparticipation'. Relative risk ratios (RRRs) were calculated using multinomial logistic regression to identify potential predictors for OS patterns. Socio-demographic, family-related, health-related, behavioural and environmental factors were considered as independent variables.
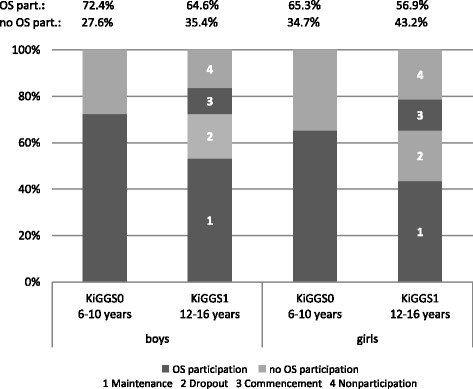
48.5 % maintained OS, 20.5 % dropped out, 12.3 % commenced OS between KiGGS0 and KiGGS1 and 18.7 % did not participate at both times. The RRRs for dropout rather than maintenance were 0.6 (95 % Cl 0.5-0.7) for boys versus girls, 1.5 (1.3-1.9) for the age group 8-10 versus 6-7 years, 0.7 (0.5-0.9) for high versus intermediate parental education, 1.4 (1.1-1.8) for low versus middle household income, 1.4 (1.0-1.8) for below-average versus average motor fitness. The RRRs for commencement rather than maintenance were 0.6 (0.5-0.8) for boys versus girls, 0.6 (0.5-0.8) for the age group 8-10 versus 6-7 years, 1.5 (1.1-2.1) for low versus intermediate parental education, 1.5 (1.1-2.0) for low versus middle household income, 0.7 (0.5-1.0) for no single-parent versus single parent family, 1.8 (1.3-2.5) for below-average and 0.6 (0.4-0.8) for above-average versus average motor fitness, and 1.4 (1.1-1.9) for high versus middle screen-based media use. The RRRs for abstinence rather than maintenance were 0.6 (0.4-0.7) for boys versus girls, 1.5 (1.1-2.0) for low versus intermediate parental education, 2.2 (1.7-2.8) for low and 0.6 (0.5-0.8) for high versus middle household income, 1.6 (1.2-2.1) for psychopathological problems versus no problems, 1.7 (1.3-2.2) for below-average and 0.4 (0.3-0.6) for above-average versus average motor fitness, and 1.6 (1.0-2.6) for rural versus metropolitan residential area.
OS participation rates among all children living in Germany need to be improved. More tailored offerings are needed which consider the preferences and interests of adolescents as well as a cooperation between public health actors to reduce barriers to OS.
有组织的体育运动(OS)参与是一项重要的健康行为,但从童年到青少年时期其参与度似乎呈下降趋势。本研究的目的是调查从童年到青少年时期的OS参与模式以及这些模式的潜在决定因素。
使用来自德国儿童和青少年健康访谈与检查调查(KiGGS)队列研究的数据,随访期为6年(KiGGS0:2003 - 2006年,KiGGS1:2009 - 2012年)。纳入KiGGS0时年龄为6 - 10岁、KiGGS1时年龄为12 - 16岁的参与者(n = 3790)。结局变量是KiGGS0和KiGGS1之间的“OS参与”,类别包括“维持参与”(参照)、“退出”、“开始参与”和“未参与”。使用多项逻辑回归计算相对风险比(RRR),以确定OS模式的潜在预测因素。社会人口学、家庭相关、健康相关、行为和环境因素被视为自变量。
在KiGGS0和KiGGS1之间,48.5%的人维持OS参与,20.5%的人退出,12.3%的人开始参与OS,18.7%的人在两个时期都未参与。与维持参与相比,退出的RRR为:男孩与女孩相比为0.6(95%CI 0.5 - 0.7);8 - 10岁年龄组与6 - 7岁年龄组相比为1.5(1.3 - 1.9);父母高学历与中等学历相比为0.7(0.5 - 0.9);低家庭收入与中等家庭收入相比为1.4(1.1 - 1.8);运动能力低于平均水平与平均水平相比为1.4(1.0 - 1.8)。与维持参与相比,开始参与的RRR为:男孩与女孩相比为0.6(0.5 - 0.8);8 - 10岁年龄组与6 - 7岁年龄组相比为0.6(0.5 - 0.8);父母低学历与中等学历相比为1.5(1.1 - 2.1);低家庭收入与中等家庭收入相比为1.5(1.1 - 2.0);非单亲家庭与单亲家庭相比为0.7(0.5 - 1.0);运动能力低于平均水平与平均水平相比为1.8(1.3 - 2.5),高于平均水平与平均水平相比为0.6(0.4 - 0.8);高屏幕媒体使用与中等屏幕媒体使用相比为1.4(1.1 - 1.9)。与维持参与相比,不参与的RRR为:男孩与女孩相比为0.