Vaidyanathan Subramanian, Samsudin Azi, Singh Gurpreet, Hughes Peter L, Soni Bakul M, Selmi Fahed
Regional Spinal Injuries Center, Southport and Formby District General Hospital, Southport, UK.
Department of Urology, Whiston Hospital, Prescot, UK.
Int Med Case Rep J. 2016 Aug 24;9:253-9. doi: 10.2147/IMCRJ.S99960. eCollection 2016.
Paraplegic patients are at greater risk of developing complications following ureteroscopic lithotripsy because of urine infection associated with neuropathic bladder, difficulties in access due to altered anatomy of urinary bladder and urethra, spinal curvature, spasticity, and contractures. We report the occurrence of large subcapsular hematoma following ureteroscopy and discuss lessons we learn from this case.
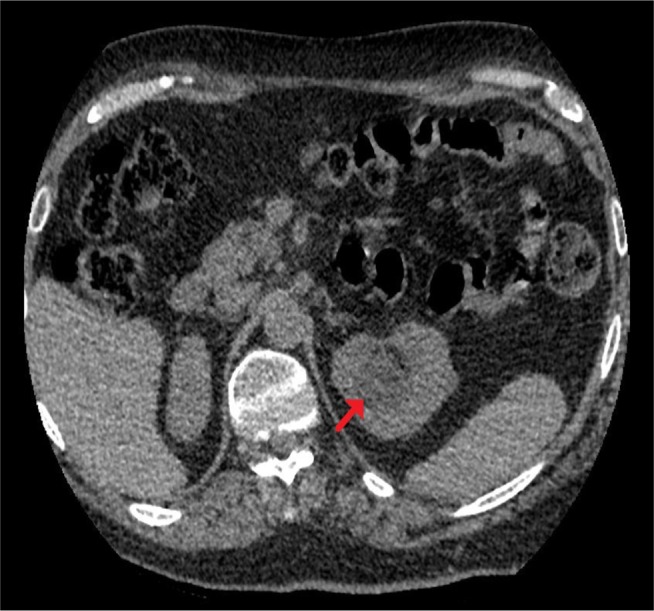
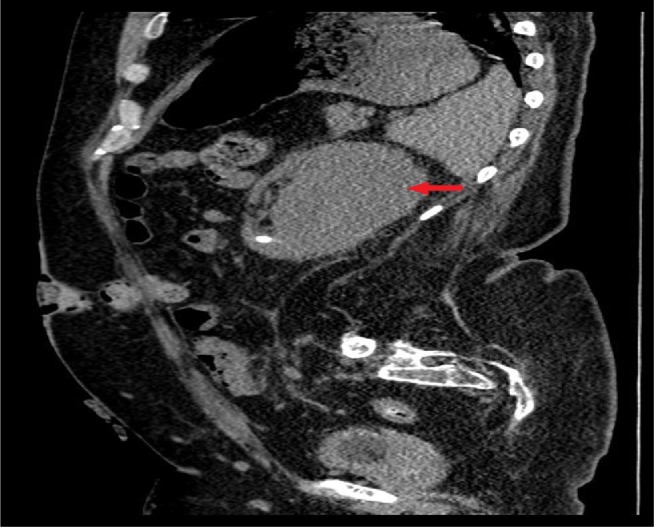
A 48-year-old male patient with spina bifida underwent ureteroscopy with laser lithotripsy and ureteric stenting for left ureteric stone and staghorn calculus with hydronephrosis; laser lithotripsy was repeated after 3 months; both procedures were performed by a senior urologist and did not result in any complications. Ureteroscopic laser lithotripsy was performed 5 months later by a urological trainee; it was difficult to negotiate the scope as vision became poor because of bleeding (as a result of the procedure). Postoperatively, hematuria persisted; temperature was 39°C. Cefuroxime was given intravenously followed by gentamicin for 5 days; hematuria subsided gradually; he was discharged home. Ten days later, this patient developed temperature, the urine culture grew Pseudomonas aeruginosa, and ciprofloxacin was given orally. Computed tomography (CT) of the urinary tract, performed 4 weeks after ureteroscopy, revealed a 9×7 cm subcapsular collection on the left kidney compressing underlying parenchyma. Percutaneous drainage was not feasible because of severe curvature of spine. Isotope renogram revealed deterioration in left renal function from 30% to 17%. Follow-up CT revealed reduction in the size of subcapsular hematoma, no hydronephrosis, and several residual calculi.
Risk of subcapsular hematoma following ureteroscopic lithotripsy can be reduced by avoiding prolonged endoscopy and performing ureteroscopy under low pressure. When a paraplegic patient develops features of infection after ureteroscopy, renal imaging should be carried out promptly. Extended perioperative medical care is required for spinal cord injury patients because of their propensity to develop sepsis. Antibiotics should be prescribed on the basis of recent urine microbiology results. Spinal cord injury patients should be treated by senior, experienced doctors and cared for in a spinal injuries unit in order to minimize complications.
截瘫患者因神经源性膀胱相关的尿液感染、膀胱和尿道解剖结构改变导致的操作困难、脊柱侧弯、痉挛和挛缩,在输尿管镜碎石术后发生并发症的风险更高。我们报告了输尿管镜检查后发生巨大肾包膜下血肿的情况,并讨论我们从该病例中学到的经验教训。
一名48岁患有脊柱裂的男性患者因左输尿管结石和鹿角形结石伴肾积水接受了输尿管镜激光碎石术和输尿管支架置入术;3个月后重复进行了激光碎石术;这两个手术均由一位资深泌尿外科医生实施,未出现任何并发症。5个月后,一名泌尿外科实习医生进行了输尿管镜激光碎石术;由于手术导致出血,视野变差,器械操作困难。术后,血尿持续存在;体温为39°C。静脉给予头孢呋辛,随后给予庆大霉素5天;血尿逐渐消退;患者出院回家。10天后,该患者出现发热,尿培养出铜绿假单胞菌,口服环丙沙星。输尿管镜检查4周后进行的泌尿系统计算机断层扫描(CT)显示左肾有一个9×7 cm的包膜下积液,压迫下方的肾实质。由于脊柱严重弯曲,无法进行经皮引流。同位素肾图显示左肾功能从30%恶化至17%。随访CT显示包膜下血肿大小减小,无肾积水,有几颗残留结石。
通过避免长时间的内镜检查和在低压下进行输尿管镜检查,可以降低输尿管镜碎石术后肾包膜下血肿的风险。当截瘫患者在输尿管镜检查后出现感染症状时,应及时进行肾脏影像学检查。由于脊髓损伤患者有发生败血症的倾向,需要延长围手术期的医疗护理。应根据近期尿液微生物学结果开具抗生素。脊髓损伤患者应由资深、有经验的医生治疗,并在脊髓损伤病房接受护理,以尽量减少并发症。