Rishi Pukhraj, Raka Neha, Rishi Ekta
Shri Bhagwan Mahavir Vitreoretinal Services, Sankara Nethralaya, Chennai, TamilNadu, India.
PLoS One. 2016 Sep 12;11(9):e0162533. doi: 10.1371/journal.pone.0162533. eCollection 2016.
To study potential ischemic effects of intravitreal Bevacizumab (IVB) on unaffected retina in treatment-naive eyes with macular edema secondary to branch retinal vein occlusion (BRVO) and contralateral eyes secondary to systemic absorption.
Prospective, interventional series included 27 treatment-naive eyes with BRVO and macular edema.
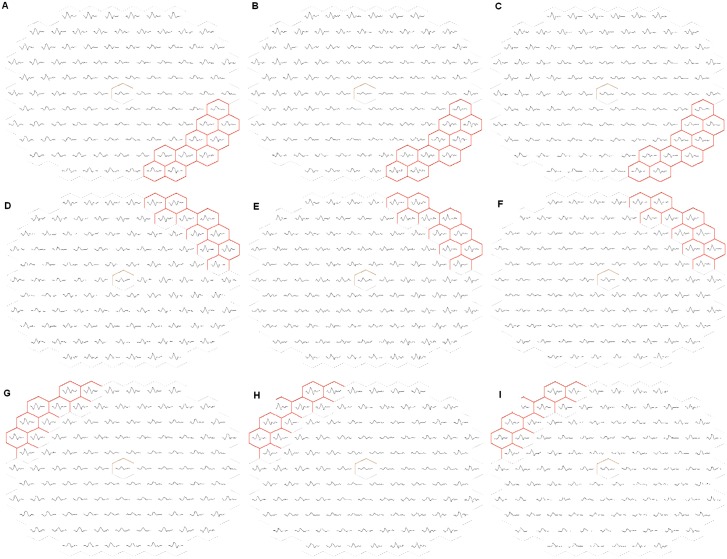
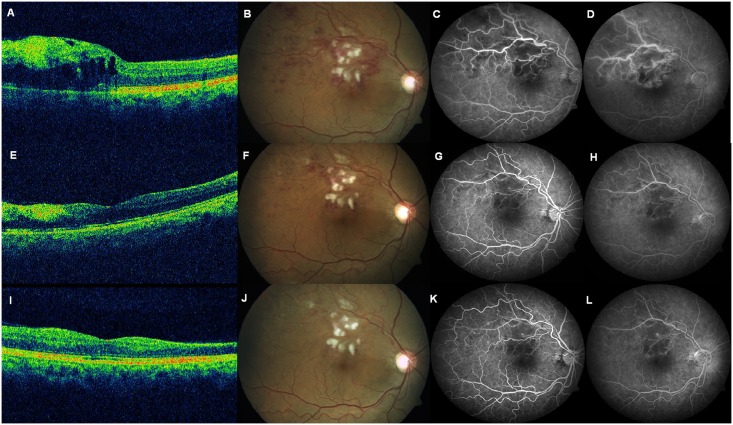
Eyes with diabetic retinopathy, glaucoma, vasculitides, papilledema or systemic neurologic condition. Subjects underwent complete ophthalmological examination including fluoroscein angiography (FA), optical coherence tomography (OCT) and multifocal electroretinogram (mf-ERG). All subjects received single 1.25 mg/0.05ml IVB injection. Two observers measured all parameters; inter-observer agreements were expressed as kappa values. Paired t-test was used to compare values at baseline and follow-up. The statistical analysis was done using SPSS for Windows, Version 14.0. (Chicago, SPSS Inc.) Presenting mean CFT (central foveal thickness) was 499.5(+/-229.7) μm, mean BCVA (best corrected visual acuity) was 0.64(+/-0.41) logMAR. At last follow-up, mean CFT was 267.9(+/-159.3) μm (P<0.001), 95% CI [127.18, 422.32]; mean BCVA was 0.28(+/-0.24) logMAR. Respectively, mean N1 and P1 amplitudes of mfERG in 'unaffected quadrant' at presentation were -6.10(+/-4.00) nV/deg2 and 17.17(+/-11.54)nV/deg2; and -5.33(+/-1.30)nV/deg2 and 15.29(+/-4.69)nV/deg2 at final follow-up (P = 0.631 and 0.197, respectively), (95% CIs [-0.93, 1.42] and [-4.22, 1.08] respectively). In fundus quadrant of fellow eyes corresponding to unaffected quadrant in treated eyes, mean N1 and P1 amplitudes at presentation were -5.39(+/-1.56)nV/deg2 and 15.89(+/-3.89)nV/deg2; and -5.39(+/-1.90)nV/deg2 and 15.9(+/-5.52)nV/deg2 (P = 0.380 and 0.208), (95% CIs [-0.57, 1.28] and [-4.1, 1.1]) at last follow-up, respectively.
This study analysed the effects with a single injection of bevacizumab. However, whether ischemic adverse effects will emerge with repeated IVB injections as a consequence of cumulative dosing needs further investigation. The setting of our study being a tertiary care centre, the numbers of fresh BRVO cases without prior intervention were limited. Thus, the limitations of our study include a small sample size with a small follow-up period. No major ocular/systemic adverse event was observed in the study period.
No evidence of progressive ischaemia attributable to single bevacizumab treatment was observed in this study. However, a larger prospective study involving subjects with cumulative dosing of bevacizumab and a longer follow-up could provide a better understanding of the potential ischaemic effects of bevacizumab or other anti-VEGF agents.
研究玻璃体内注射贝伐单抗(IVB)对初治的视网膜分支静脉阻塞(BRVO)继发黄斑水肿患眼及对侧眼未受影响视网膜的潜在缺血性影响,以及全身吸收的情况。
前瞻性干预系列研究纳入了27例初治的BRVO继发黄斑水肿患眼。
患有糖尿病性视网膜病变、青光眼、血管炎、视乳头水肿或全身性神经系统疾病的眼。受试者接受了包括荧光素血管造影(FA)、光学相干断层扫描(OCT)和多焦视网膜电图(mf-ERG)在内的全面眼科检查。所有受试者均接受了单次1.25mg/0.05ml的IVB注射。两名观察者测量所有参数;观察者间一致性用kappa值表示。配对t检验用于比较基线和随访时的值。使用SPSS for Windows 14.0版(芝加哥,SPSS公司)进行统计分析。呈现的平均中心凹厚度(CFT)为499.5(±229.7)μm,平均最佳矫正视力(BCVA)为0.64(±0.41)logMAR。在最后一次随访时,平均CFT为267.9(±159.3)μm(P<0.001),95%置信区间[127.18, 422.32];平均BCVA为0.28(±0.24)logMAR。在初诊时,“未受影响象限”的mfERG平均N1和P1振幅分别为-6.10(±4.00)nV/deg2和17.17(±11.54)nV/deg2;在最后一次随访时分别为-5.33(±1.30)nV/deg2和15.29(±4.69)nV/deg2(P分别为0.631和0.197),(95%置信区间分别为[-0.93, 1.42]和[-4.22, 1.08])。在治疗眼未受影响象限对应的对侧眼眼底象限,初诊时平均N1和P1振幅分别为-5.39(±1.56)nV/deg2和15.89(±3.89)nV/deg2;在最后一次随访时分别为-5.39(±1.90)nV/deg2和15.9(±5.52)nV/deg2(P分别为0.380和0.208),(95%置信区间分别为[-0.57, 1.28]和[-4.1, 1.1])。
本研究分析了单次注射贝伐单抗的效果。然而,由于累积给药,重复IVB注射是否会出现缺血性不良反应需要进一步研究。我们的研究是在三级医疗中心进行的,未经事先干预 的新鲜BRVO病例数量有限。因此,我们研究的局限性包括样本量小和随访期短。在研究期间未观察到重大眼/全身不良事件。
本研究未观察到单次贝伐单抗治疗导致进行性缺血的证据。然而,一项涉及贝伐单抗累积给药受试者且随访期更长的更大规模前瞻性研究,可能会更好地了解贝伐单抗或其他抗VEGF药物的潜在缺血性影响。