Department of Ophthalmology, Queen's University, Kingston, ON, Canada.
BMJ. 2012 Jul 4;345:e4203. doi: 10.1136/bmj.e4203.
To assess the risk of systemic adverse events associated with intravitreal injections of vascular endothelial growth factor inhibiting drugs.
Population based nested case-control study.
Ontario, Canada.
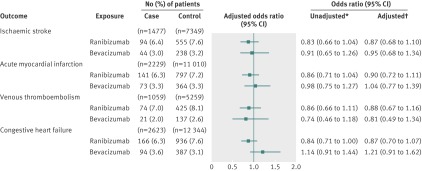
91,378 older adults with a history of physician diagnosed retinal disease identified between 1 April 2006 and 31 March 2011. Cases were 1477 patients admitted to hospital for ischaemic stroke, 2229 admitted for an acute myocardial infarction, 1059 admitted or assessed in an emergency department for venous thromboembolism, and 2623 admitted for congestive heart failure. Event-free controls (at a ratio of 5:1) were matched to cases on the basis of year of birth, sex, history of the outcome in the previous 5 years, and diabetes.
Exposure to vascular endothelial growth factor inhibiting drugs identified within 180 days before the index date.
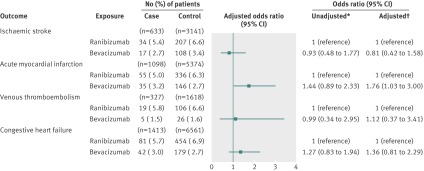
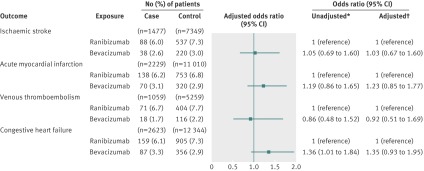
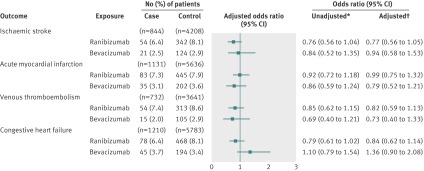
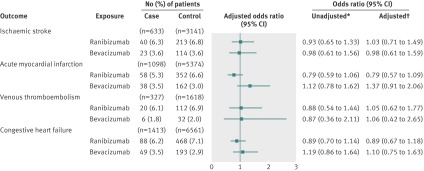
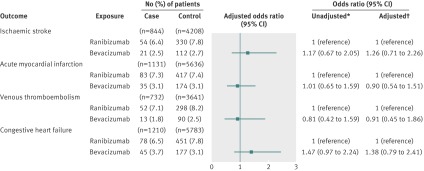
After adjustment for potential confounders, participants who had ischaemic stroke, acute myocardial infarction, congestive heart failure, or venous thromboembolism were not more likely than control participants to have been exposed to either bevacizumab (adjusted odds ratios of 0.95 (95% confidence interval 0.68 to 1.34) for ischaemic stroke, 1.04 (0.77 to 1.39) for acute myocardial infarction, 0.81 (0.49 to 1.34) for venous thromboembolism, and 1.21 (0.91 to 1.62) for congestive heart failure) or ranibizumab (adjusted odds ratios 0.87 (0.68 to 1.10) for ischaemic stroke, 0.90 (0.72 to 1.11) for acute myocardial infarction, 0.88 (0.67 to 1.16) for venous thromboembolism, and 0.87 (0.70 to 1.07) for congestive heart failure). Similarly, a secondary analysis of exclusive users of bevacizumab or ranibizumab showed no differences in risk between the two drugs (adjusted odds ratios for bevacizumab relative to ranibizumab of 1.03 (0.67 to 1.60) for ischaemic stroke, 1.23 (0.85 to 1.77) for acute myocardial infarction, 0.92 (0.51 to 1.69) for venous thromboembolism, and 1.35 (0.93 to 1.95) for congestive heart failure). These findings were consistent for all but one outcome in subgroup analyses.
Intravitreal injections of bevacizumab and ranibizumab were not associated with significant risks of ischaemic stroke, acute myocardial infarction, congestive heart failure, or venous thromboembolism.
评估与血管内皮生长因子抑制药物玻璃体腔内注射相关的全身不良事件的风险。
基于人群的巢式病例对照研究。
加拿大安大略省。
91378 名年龄在 40 岁以上、有医生诊断的视网膜疾病史的成年人,他们于 2006 年 4 月 1 日至 2011 年 3 月 31 日期间被确定。病例是因缺血性中风住院的 1477 名患者、因急性心肌梗死住院的 2229 名患者、因静脉血栓栓塞症在急诊室住院或接受评估的 1059 名患者、因充血性心力衰竭住院的 2623 名患者。根据出生年份、性别、前 5 年的结局史和糖尿病,将无事件对照组(5:1 匹配)与病例相匹配。
在指数日期前 180 天内接触血管内皮生长因子抑制药物。
在调整了潜在混杂因素后,与对照组相比,缺血性中风、急性心肌梗死、充血性心力衰竭或静脉血栓栓塞症患者接受贝伐单抗(缺血性中风的调整后比值比为 0.95(95%置信区间为 0.68 至 1.34)、急性心肌梗死为 1.04(0.77 至 1.39)、静脉血栓栓塞症为 0.81(0.49 至 1.34)、充血性心力衰竭为 1.21(0.91 至 1.62))或雷珠单抗(缺血性中风的调整后比值比为 0.87(0.68 至 1.10)、急性心肌梗死为 0.90(0.72 至 1.11)、静脉血栓栓塞症为 0.88(0.67 至 1.16)、充血性心力衰竭为 0.87(0.70 至 1.07))的可能性并不更高。同样,对贝伐单抗或雷珠单抗的纯使用者的二次分析显示,两种药物之间的风险没有差异(贝伐单抗相对于雷珠单抗的调整比值比为缺血性中风为 1.03(0.67 至 1.60)、急性心肌梗死为 1.23(0.85 至 1.77)、静脉血栓栓塞症为 0.92(0.51 至 1.69)、充血性心力衰竭为 1.35(0.93 至 1.95))。这些发现除了一个结局的亚组分析外,在其他所有情况下都是一致的。
玻璃体腔内注射贝伐单抗和雷珠单抗与缺血性中风、急性心肌梗死、充血性心力衰竭或静脉血栓栓塞症的显著风险无关。