Burnett A K, Russell N H, Hills R K, Kell J, Nielsen O J, Dennis M, Cahalin P, Pocock C, Ali S, Burns S, Freeman S, Milligan D, Clark R E
Department of Haematology, Cardiff University School of Medicine, Cardiff, UK.
Department of Haematology, Nottingham University Hospital NHS Trust, Nottingham, UK.
Leukemia. 2017 Feb;31(2):310-317. doi: 10.1038/leu.2016.225. Epub 2016 Sep 2.
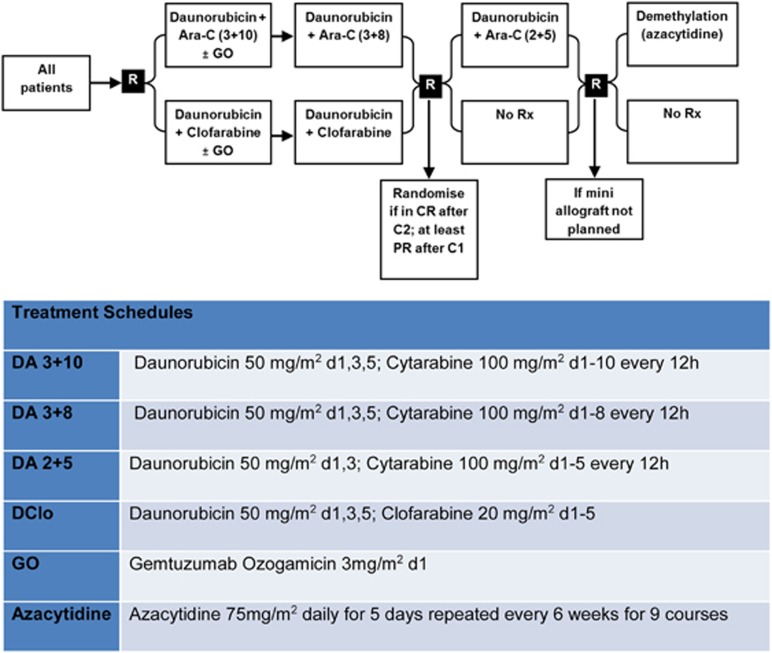
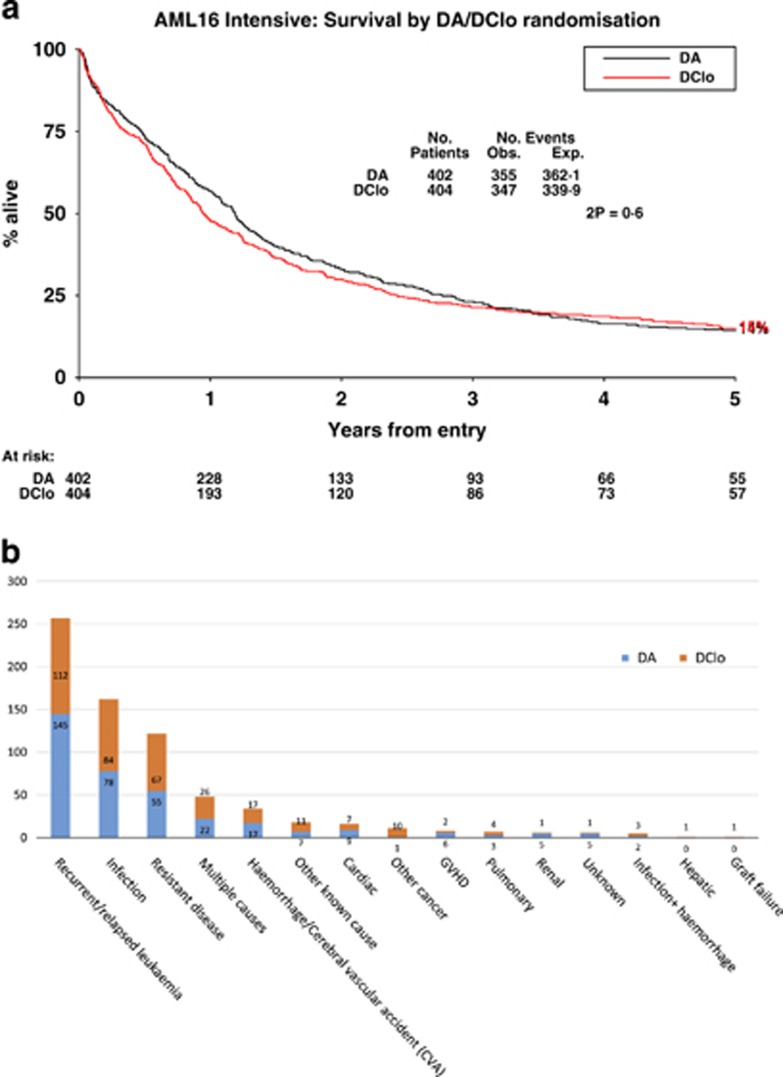
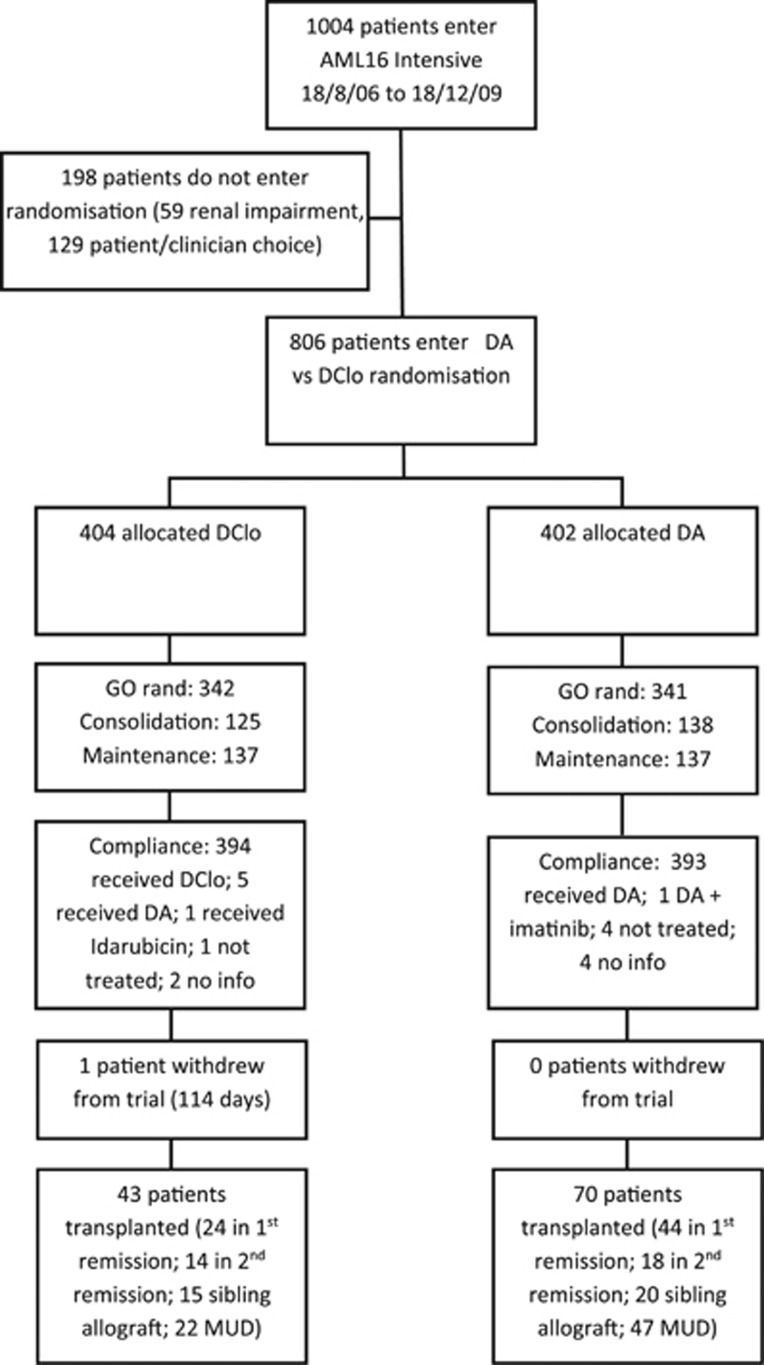
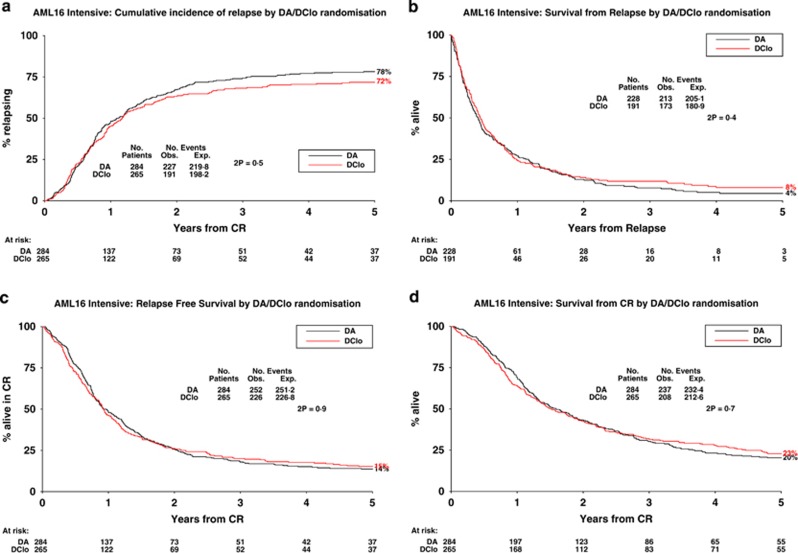
The study was designed to compare clofarabine plus daunorubicin vs daunorubicin/ara-C in older patients with acute myeloid leukaemia (AML) or high-risk myelodysplastic syndrome (MDS). Eight hundred and six untreated patients in the UK NCRI AML16 trial with AML/high-risk MDS (median age, 67 years; range 56-84) and normal serum creatinine were randomised to two courses of induction chemotherapy with either daunorubicin/ara-C (DA) or daunorubicin/clofarabine (DClo). Patients were also included in additional randomisations; ± one dose of gemtuzumab ozogamicin in course 1; 2v3 courses and ± azacitidine maintenance. The primary end point was overall survival. The overall response rate was 69% (complete remission (CR) 60%; CRi 9%), with no difference between DA (71%) and DClo (66%). There was no difference in 30-/60-day mortality or toxicity: significantly more supportive care was required in the DA arm even though platelet and neutrophil recovery was significantly slower with DClo. There were no differences in cumulative incidence of relapse (74% vs 68%; hazard ratio (HR) 0.93 (0.77-1.14), P=0.5); survival from relapse (7% vs 9%; HR 0.96 (0.77-1.19), P=0.7); relapse-free (31% vs 32%; HR 1.02 (0.83-1.24), P=0.9) or overall survival (23% vs 22%; HR 1.08 (0.93-1.26), P=0.3). Clofarabine 20 mg/m given for 5 days with daunorubicin is not superior to ara-C+daunorubicin as induction for older patients with AML/high-risk MDS.
该研究旨在比较氯法拉滨联合柔红霉素与柔红霉素/阿糖胞苷用于老年急性髓系白血病(AML)或高危骨髓增生异常综合征(MDS)患者的疗效。英国国家癌症研究所AML16试验中的806例未经治疗的AML/高危MDS患者(中位年龄67岁;范围56 - 84岁)且血清肌酐正常,被随机分为两组,分别接受柔红霉素/阿糖胞苷(DA)或柔红霉素/氯法拉滨(DClo)进行两个疗程的诱导化疗。患者还被纳入其他随机分组;第1疗程±一剂吉妥珠单抗奥佐米星;2个疗程与3个疗程对比以及±阿扎胞苷维持治疗。主要终点是总生存期。总缓解率为69%(完全缓解(CR)60%;部分缓解(CRi)9%),DA组(71%)和DClo组(66%)之间无差异。30天/60天死亡率或毒性方面无差异:尽管DClo组血小板和中性粒细胞恢复明显较慢,但DA组需要更多的支持治疗。复发的累积发生率(74%对68%;风险比(HR)0.93(0.77 - 1.14),P = 0.5)、复发后的生存期(7%对9%;HR 0.96(0.77 - 1.19),P = 0.7)、无复发生存期(31%对32%;HR 1.02(0.83 - 1.24),P = 0.9)或总生存期(23%对22%;HR 1.08(0.93 - 1.26),P = 0.3)均无差异。对于老年AML/高危MDS患者,氯法拉滨20mg/m²给药5天联合柔红霉素作为诱导治疗并不优于阿糖胞苷+柔红霉素。