Brown Merritt Weaver, Yilmaz Tülin Serap, Kasper Ekkehard M
Department of Neurology, Beth Israel Deaconess Medical Center, Boston, MA, USA.
Department of Neurosurgery, Beth Israel Deaconess Medical Center, Boston, MA, USA.
Surg Neurol Int. 2016 Aug 29;7(Suppl 22):S581-9. doi: 10.4103/2152-7806.189441. eCollection 2016.
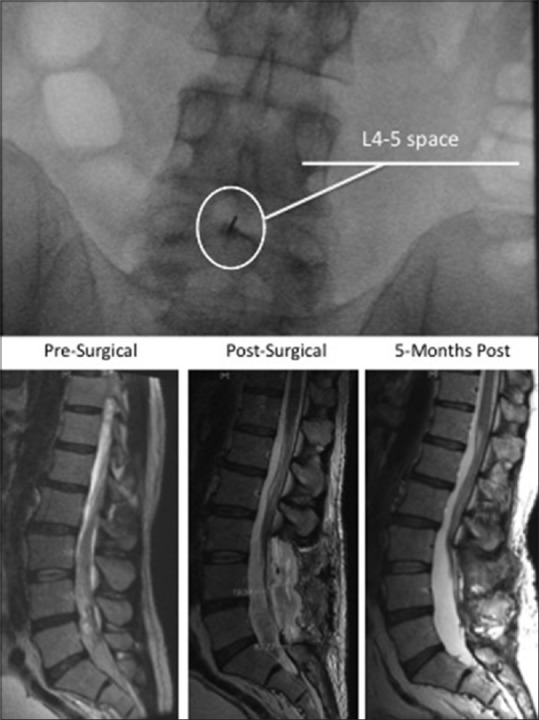
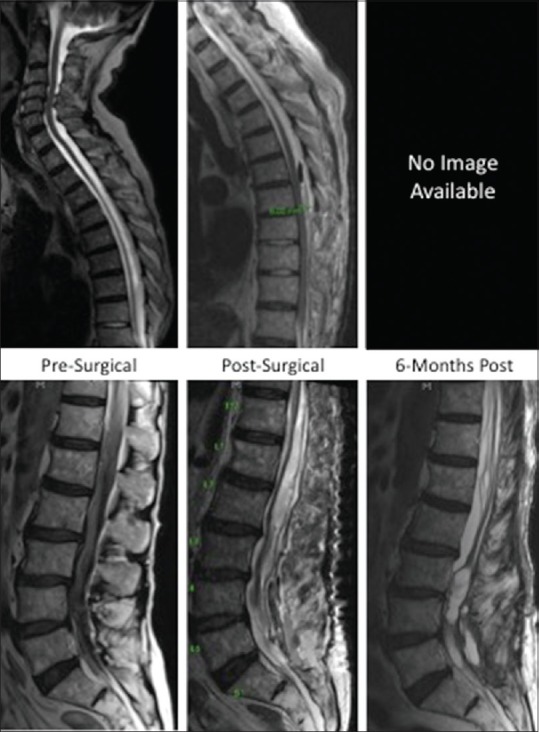
Lumbar puncture (LP) rarely results in complications such as spinal hematomas. However, it remains unclear if certain variables increase likelihood of these events, or if surgical intervention improves outcome.
In addition to two clinical vignettes, we evaluated the post-1974 literature for cases of spinal hematoma and subsequent intervention. Based on our compilation of data, we evaluated outcome relative to numerous distinct variables.
Based on 35 LP-related spinal hematoma cases in the post-1974 literature and our encounters, we found 28.6% of patients presenting with preexisting coagulopathy had poor outcomes regardless of intervention, relative to 14.3% of patients without coagulopathy; a highly significant difference (P = 0.02). Once diagnosed, 21 patients were treated surgically and 14 nonsurgically. Of the 60% surgical patients, 57.1% had good outcomes, and 42.9% had poor outcomes within 12 months. Of 40% nonsurgical patients, 57.1% had good outcomes and 42.9% had poor outcomes. Results in these groups were not statistically different.
We found a significant correlation between preexisting coagulopathy and poor neurological outcome irrespective of intervention. However, outcomes for these patients may be confounded by comorbidities including underlying conditions contributing to their coagulopathy. No significant correlation between type of surgical intervention and good outcome was found, possibly attributable to the paucity of details in existing case reports and the difficulty defining the degree of spinal cord compromise from a given lesion. Despite our findings, emergent neurosurgical intervention may be beneficial for the management of complications such as cauda equina syndrome secondary to intrathecal spinal hematoma.
腰椎穿刺(LP)很少导致诸如脊髓血肿等并发症。然而,目前尚不清楚某些变量是否会增加这些事件的发生可能性,或者手术干预是否能改善预后。
除了两个临床案例,我们评估了1974年以后关于脊髓血肿病例及后续干预的文献。基于我们汇总的数据,我们评估了与众多不同变量相关的预后情况。
根据1974年以后文献中的35例与LP相关的脊髓血肿病例以及我们遇到的病例,我们发现,无论是否进行干预,28.6%患有凝血功能障碍的患者预后较差,而无凝血功能障碍的患者这一比例为14.3%;差异具有高度统计学意义(P = 0.02)。一旦确诊,21例患者接受了手术治疗,14例接受了非手术治疗。在接受手术治疗的60%患者中,57.1%在12个月内预后良好,42.9%预后较差。在接受非手术治疗的40%患者中,57.1%预后良好,42.9%预后较差。这些组的结果在统计学上没有差异。
我们发现,无论是否进行干预,既往存在的凝血功能障碍与不良神经学预后之间存在显著相关性。然而,这些患者的预后可能会受到合并症的影响,包括导致其凝血功能障碍的基础疾病。未发现手术干预类型与良好预后之间存在显著相关性,这可能归因于现有病例报告中细节不足,以及难以从给定病变确定脊髓受压程度。尽管我们有这些发现,但紧急神经外科干预可能有利于管理诸如鞘内脊髓血肿继发的马尾综合征等并发症。