Bang Cæcilie Larsen, Porsbjerg Celeste Michala
Department of Lung medicine, Bispebjerg University Hospital, Denmark.
Respir Med Case Rep. 2016 Aug 20;19:94-7. doi: 10.1016/j.rmcr.2016.08.004. eCollection 2016.
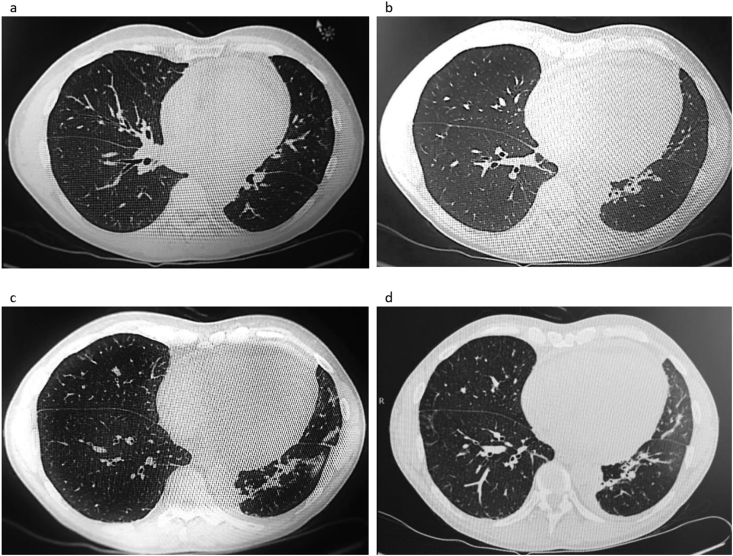
Heart involvement is the most critical and potentially lethal systemic manifestation in eosinophilic granulomatosis with polyangiitis (EGPA). We present a case of acute chest pain in a 58-year-old male with severe asthma, which regressed after sublingual administration of nitroglycerine. At the time of hospital admission, there were non-specific ST-changes on the ecg, coronary enzymes were increased, and the patient was concluded to have a non-ST-elevation myocardial infarction, and treated as such. A subacute cardiac catheterization showed no signs of significant coronary stenosis. During the next days, there was increasing pain and reduced strength in both feet. Paraclinical imaging and neurological examinations could not explain the symptoms, and physiotherapy was initiated. At the time, no connection to patient's diagnosis of severe asthma was made. The patient was seen in the respiratory outpatient clinic for a routine check-up, three weeks after the initial hospital admission. At this point, there was increasing pain in both legs and the patient had difficulty walking and experienced increasing dyspnea. Blood eosinophils were elevated (12.7 × 10(9)/L), and an acute HRCT scan showed bilateral peribronchial infiltrates with ground glass opacification and small noduli. A diagnosis of EGPA was established, and administration of systemic glucocorticoids was initiated. A year and a half later, there is still reduced strength and sensory loss. This case illustrates that it is important to consider alternative diagnoses in patients with atypical symptoms and a low risk profile. Heart involvement is the most critical and potentially lethal systemic manifestation in eosinophilic granulomatosis with polyangiitis (EGPA, formerly known as Churg-Strauss syndrome), which makes a quick diagnosis and prompt initiation of correct treatment imperative.
心脏受累是嗜酸性肉芽肿性多血管炎(EGPA)最关键且可能致命的全身表现。我们报告一例58岁患有严重哮喘的男性急性胸痛病例,该患者舌下含服硝酸甘油后症状缓解。入院时,心电图有非特异性ST段改变,心肌酶升高,患者被诊断为非ST段抬高型心肌梗死并接受相应治疗。亚急性心脏导管检查未显示明显冠状动脉狭窄迹象。在接下来的几天里,患者双脚疼痛加剧且力量减弱。辅助检查成像和神经学检查均无法解释这些症状,于是开始进行物理治疗。当时,未将这些症状与患者的严重哮喘诊断联系起来。首次入院三周后,患者到呼吸门诊进行常规检查。此时,患者双腿疼痛加剧,行走困难且呼吸困难加重。血液嗜酸性粒细胞升高(12.7×10⁹/L),急性高分辨率CT扫描显示双侧支气管周围浸润伴磨玻璃样混浊和小结节。确诊为EGPA,并开始给予全身糖皮质激素治疗。一年半后,患者仍存在力量减弱和感觉丧失的情况。该病例表明,对于症状不典型且风险较低的患者,考虑其他诊断很重要。心脏受累是嗜酸性肉芽肿性多血管炎(EGPA,以前称为Churg-Strauss综合征)最关键且可能致命的全身表现,这使得快速诊断并及时开始正确治疗势在必行。