Driessen Sara R C, Wallwiener Markus, Taran Florin-Andrei, Cohen Sarah L, Kraemer Bernhard, Wallwiener Christian W, van Zwet Erik W, Brucker Sara Y, Jansen Frank Willem
Department of Gynecology, Leiden University Medical Center, PO Box 9600, 2300 RC, Leiden, The Netherlands.
Department of Obstetrics and Gynecology, University of Heidelberg, INF 440, 69115, Heidelberg, Germany.
Arch Gynecol Obstet. 2017 Jan;295(1):111-117. doi: 10.1007/s00404-016-4199-2. Epub 2016 Sep 15.
To compare hospital versus individual surgeon's perioperative outcomes for laparoscopic hysterectomy (LH), and to assess the relationship between surgeon experience and perioperative outcomes.
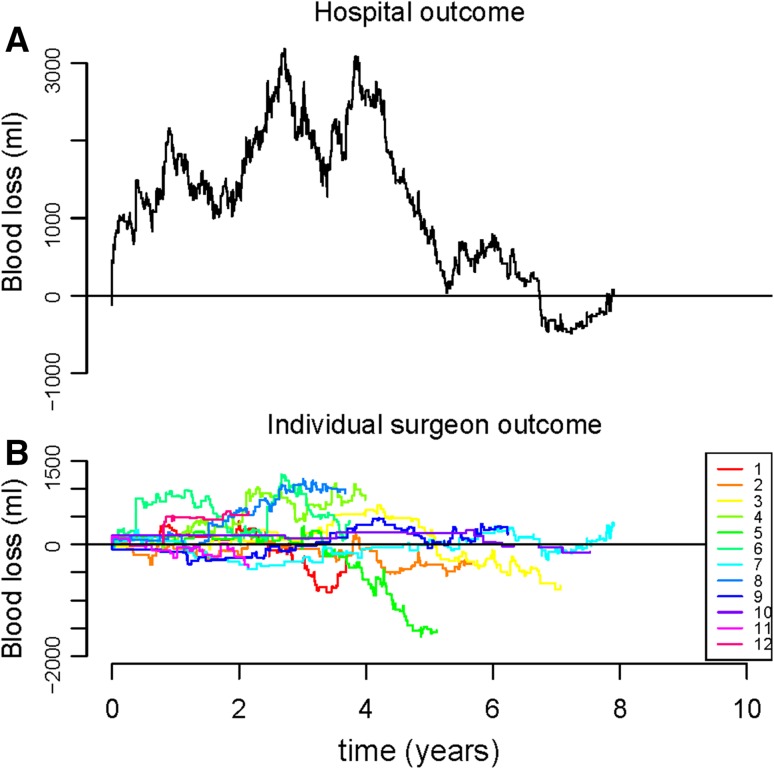
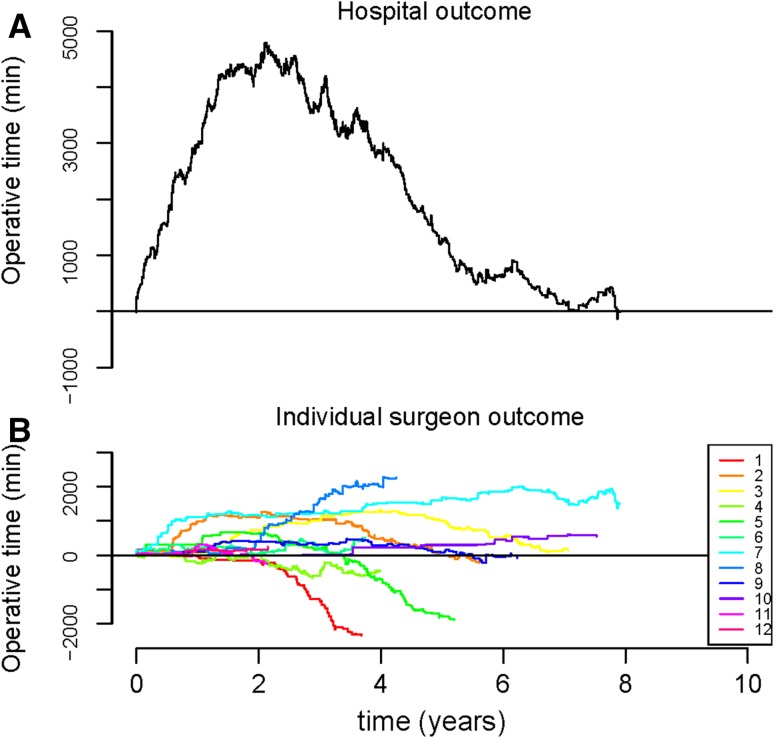
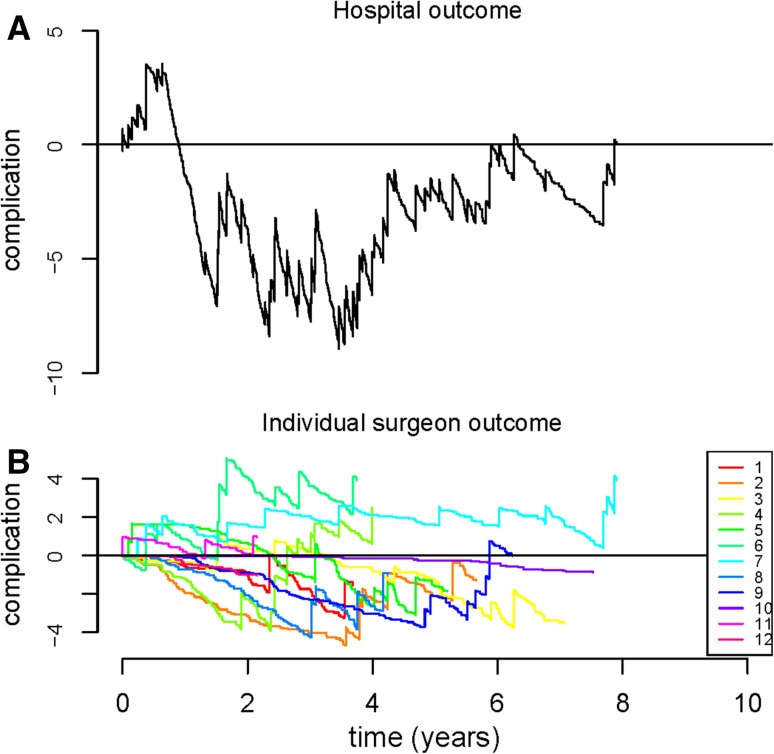
A retrospective analysis of all prospective collected LHs performed from 2003 to 2010 at one medical center was performed. Perioperative outcomes (operative time, blood loss, complication rate) were assessed on both a hospital level and surgeon level using Cumulative Observed minus Expected performance graphs.
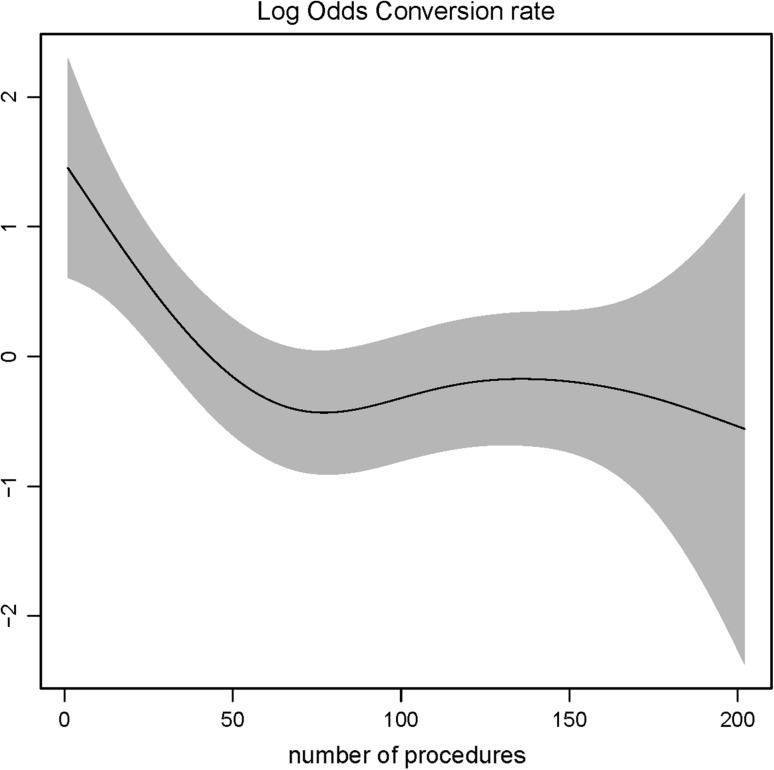
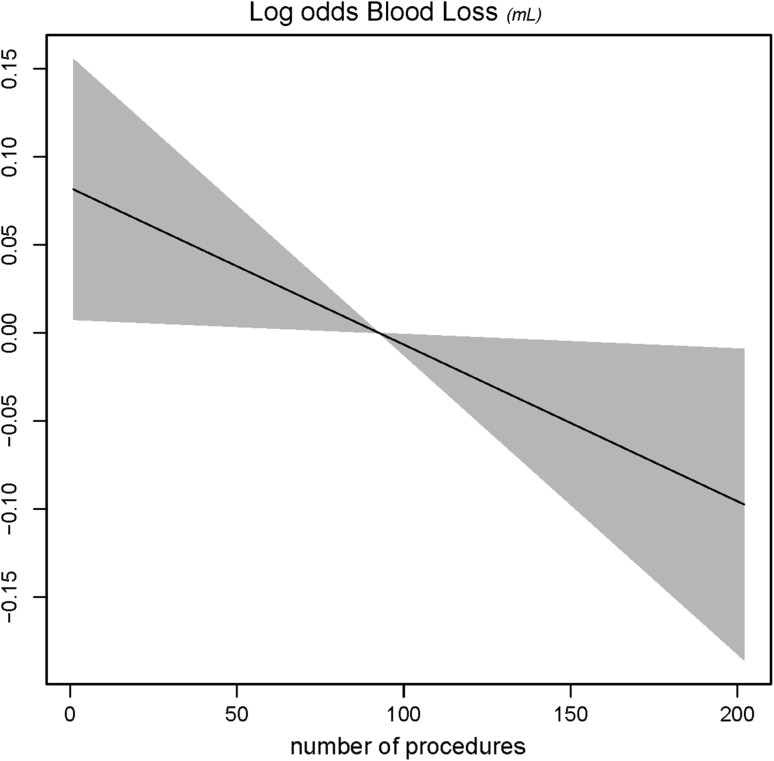
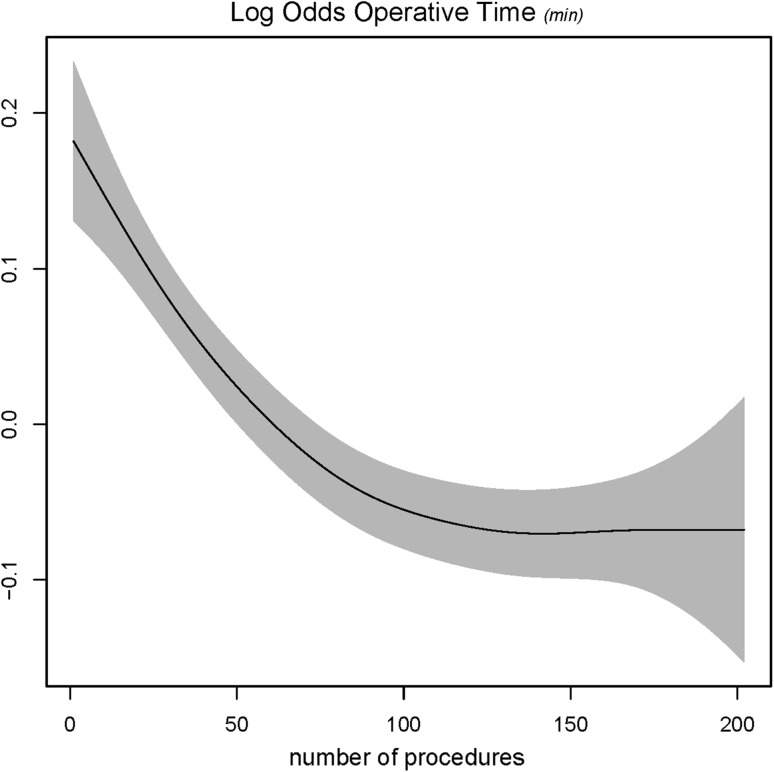
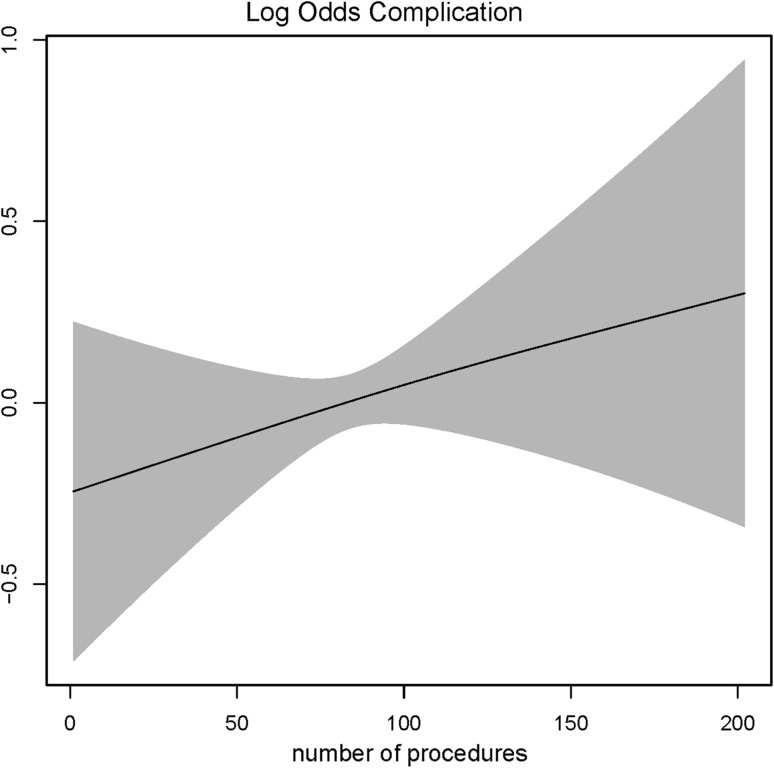
A total of 1618 LHs were performed, 16 % total laparoscopic hysterectomies and 84 % laparoscopic supracervical hysterectomies. Overall outcomes included mean (SD±) blood loss 108.9 ± 69.2 mL, mean operative time 95.4 ± 39.7 min and a complication occurred in 76 (4.7 %) of cases. Suboptimal perioperative outcomes of an individual surgeon were not always detected on a hospital level. However, collective suboptimal outcomes were faster detected on a hospital level compared to individual surgeon's level. Evidence of a learning curve is seen; for the first 100 procedures, a decrease in operative time is observed as individual surgeon experience increases. Similarly, the risk of conversion decreases up to the first 50 procedures.
An individual outlier (i.e., surgeon with consistently suboptimal performance) will not always be detected when monitoring outcome measures only on a hospital level. However, monitoring outcome measures on a hospital level will detect suboptimal performance earlier compared to monitoring only on an individual surgeon's level. To detect performance outliers timely, insight into an individual surgeon's outcome and skills is recommended. Furthermore, an experienced surgeon is no guarantee for acceptable surgical outcomes.
比较腹腔镜子宫切除术(LH)在医院层面与个体外科医生的围手术期结局,并评估外科医生经验与围手术期结局之间的关系。
对2003年至2010年在某医疗中心进行的所有前瞻性收集的LH手术进行回顾性分析。使用累积观察减去预期性能图在医院层面和外科医生层面评估围手术期结局(手术时间、失血量、并发症发生率)。
共进行了1618例LH手术,其中全腹腔镜子宫切除术占16%,腹腔镜次全子宫切除术占84%。总体结局包括平均(标准差±)失血量108.9±69.2 mL,平均手术时间95.4±39.7分钟,76例(4.7%)发生并发症。个体外科医生的围手术期结局不理想在医院层面并不总是能被检测到。然而,与个体外科医生层面相比,医院层面能更快检测到总体不理想的结局。可见学习曲线的证据;在前100例手术中,随着个体外科医生经验的增加,手术时间有所减少。同样,在最初的50例手术中,中转风险也会降低。
仅在医院层面监测结局指标时,个体异常值(即表现持续不理想的外科医生)并不总是能被检测到。然而,与仅在个体外科医生层面监测相比,在医院层面监测结局指标能更早发现不理想的表现。为了及时发现表现异常者,建议深入了解个体外科医生的结局和技能。此外,经验丰富的外科医生并不能保证手术结局可接受。