Emilsson Össur Ingi, Benediktsdóttir Bryndís, Ólafsson Ísleifur, Cook Elizabeth, Júlíusson Sigurður, Björnsson Einar Stefán, Guðlaugsdóttir Sunna, Guðmundsdóttir Anna Soffía, Mirgorodskaya Ekaterina, Ljungström Evert, Arnardóttir Erna Sif, Gíslason Thórarinn, Janson Christer, Olin Anna-Carin
Faculty of Medicine, University of Iceland, Vatnsmyrarvegur 16, 101, Reykjavik, Iceland.
Department of Respiratory Medicine and Sleep, Landspitali University Hospital, Reykjavik, Iceland.
Respir Res. 2016 Sep 20;17(1):115. doi: 10.1186/s12931-016-0431-7.
Nocturnal gastroesophageal reflux (nGER) is associated with respiratory symptoms and sleep-disordered breathing (SDB), but the pathogenesis is unclear. We aimed to investigate the association between nGER and respiratory symptoms, exacerbations of respiratory symptoms, SDB and airway inflammation.
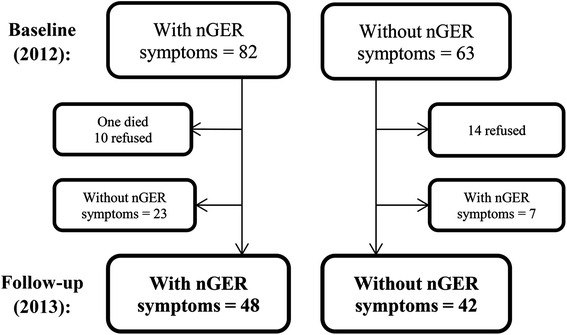
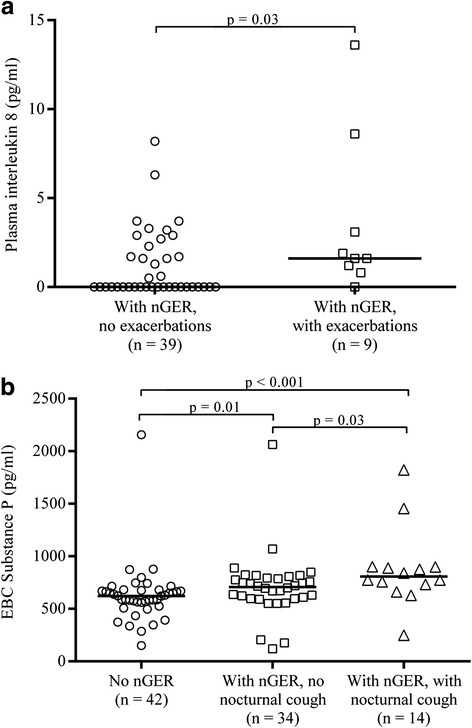
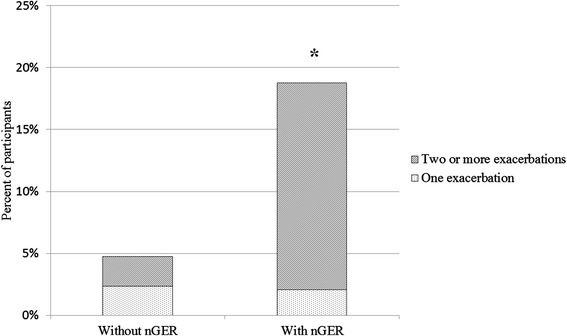
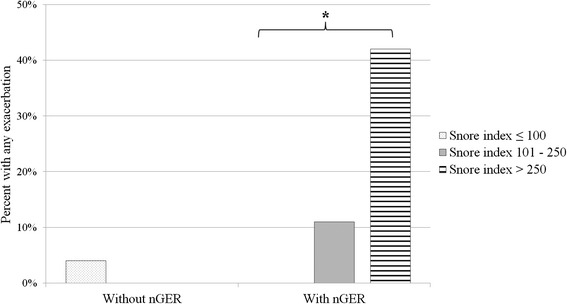
Participants in the European Community Respiratory Health Survey III in Iceland with nGER symptoms (n = 48) and age and gender matched controls (n = 42) were studied by questionnaires, exhaled breath condensate (EBC), particles in exhaled air (PEx) measurements, and a home polygraphic study. An exacerbation of respiratory symptoms was defined as an episode of markedly worse respiratory symptoms in the previous 12 months.
Asthma and bronchitis symptoms were more common among nGER subjects than controls (54 % vs 29 %, p = 0.01; and 60 % vs 26 %, p < 0.01, respectively), as were exacerbations of respiratory symptoms (19 % vs 5 %, p = 0.04). Objectively measured snoring was more common among subjects with nGER than controls (snores per hour of sleep, median (IQR): 177 (79-281) vs 67 (32-182), p = 0.004). Pepsin (2.5 ng/ml (0.8-5.8) vs 0.8 ng/ml (0.8-3.6), p = 0.03), substance P (741 pg/ml (626-821) vs 623 pg/ml (562-676), p < 0.001) and 8-isoprostane (3.0 pg/ml (2.7-3.9) vs 2.6 pg/ml (2.2-2.9), p = 0.002) in EBC were higher among nGER subjects than controls. Albumin and surfactant protein A in PEx were lower among nGER subjects. These findings were independent of BMI.
In a general population sample, nGER is associated with symptoms of asthma and bronchitis, as well as exacerbations of respiratory symptoms. Also, nGER is associated with increased respiratory effort during sleep. Biomarker measurements in EBC, PEx and serum indicate that micro-aspiration and neurogenic inflammation are plausible mechanisms.
夜间胃食管反流(nGER)与呼吸道症状和睡眠呼吸紊乱(SDB)相关,但其发病机制尚不清楚。我们旨在研究nGER与呼吸道症状、呼吸道症状加重、SDB和气道炎症之间的关联。
通过问卷调查、呼出气冷凝物(EBC)、呼出气颗粒(PEx)测量以及家庭多导睡眠监测研究冰岛欧洲共同体呼吸健康调查III中出现nGER症状的参与者(n = 48)以及年龄和性别匹配的对照组(n = 42)。呼吸道症状加重被定义为在过去12个月中呼吸道症状明显恶化的发作。
nGER受试者中哮喘和支气管炎症状比对照组更常见(分别为54%对29%,p = 0.01;以及60%对26%,p < 0.01),呼吸道症状加重情况也是如此(19%对5%,p = 0.04)。客观测量的打鼾在nGER受试者中比对照组更常见(每小时睡眠打鼾次数,中位数(IQR):177(79 - 281)对67(32 - 182),p = 0.004)。nGER受试者EBC中的胃蛋白酶(2.5 ng/ml(0.8 - 5.8)对0.8 ng/ml(0.8 - 3.6),p = 0.03)、P物质(741 pg/ml(626 - 821)对623 pg/ml(562 - 676),p < 0.001)和8 - 异前列腺素(3.0 pg/ml(2.7 - 3.9)对2.6 pg/ml(2.2 - 2.9),p = 0.002)高于对照组。nGER受试者PEx中的白蛋白和表面活性蛋白A较低。这些发现与体重指数无关。
在一般人群样本中,nGER与哮喘和支气管炎症状以及呼吸道症状加重相关。此外,nGER与睡眠期间呼吸努力增加有关。EBC、PEx和血清中的生物标志物测量表明微误吸和神经源性炎症是合理的机制。