Donatelli Gianfranco, Cereatti Fabrizio, Dumont Jean-Loup, Dhumane Parag, Tuszynski Thierry, Derhy Serge, Meduri Alexandre, Vergeau Bertrand Marie, Meduri Bruno
Unité d'Endoscopie Interventionnelle, Ramsay Générale de Santé, Hôpital Privé des Peupliers, Paris, France.
Unit of Interventional Endoscopy, Department of General Surgery "P. Stefanini", "Sapienza" University of Rome, Rome, Italy.
Endosc Int Open. 2016 Sep;4(9):E957-63. doi: 10.1055/s-0042-107070. Epub 2016 May 12.
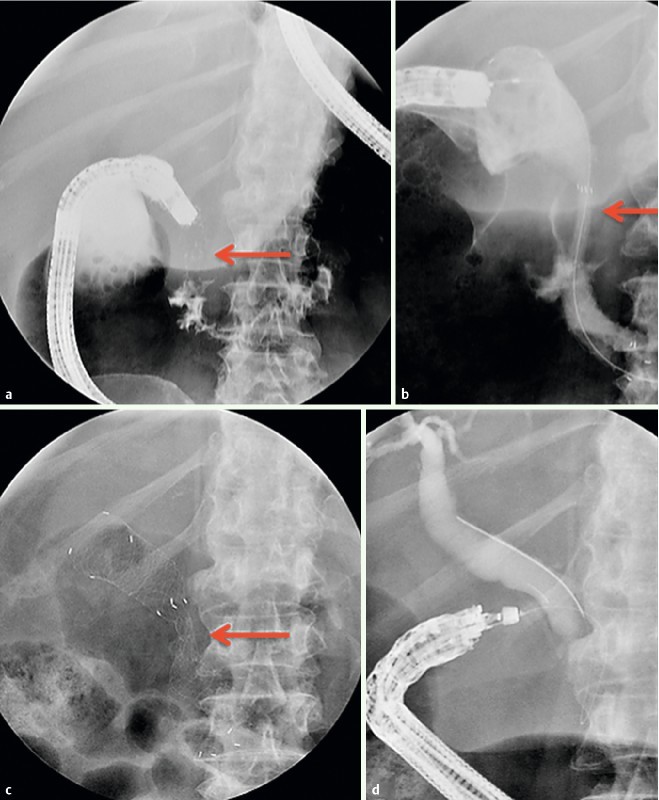
Duodenal obstruction may prevent performance of endoscopic retrograde cholangiopancreatography (ERCP). Percutaneous transhepatic biliary drainage (PTBD) or Endoscopic ultrasonograhy-guided biliary access (EUS-BD) are alternative treatments but are associated with a higher morbidity and mortality rate. The aim of the study is to report overall technical success rate and clinical outcome with deployment of temporary fully or partially covered self-expanding duodenal stent (pc/fcSEMS) as a bridge to ERCP in case of inaccessible papilla due to duodenal strictures.
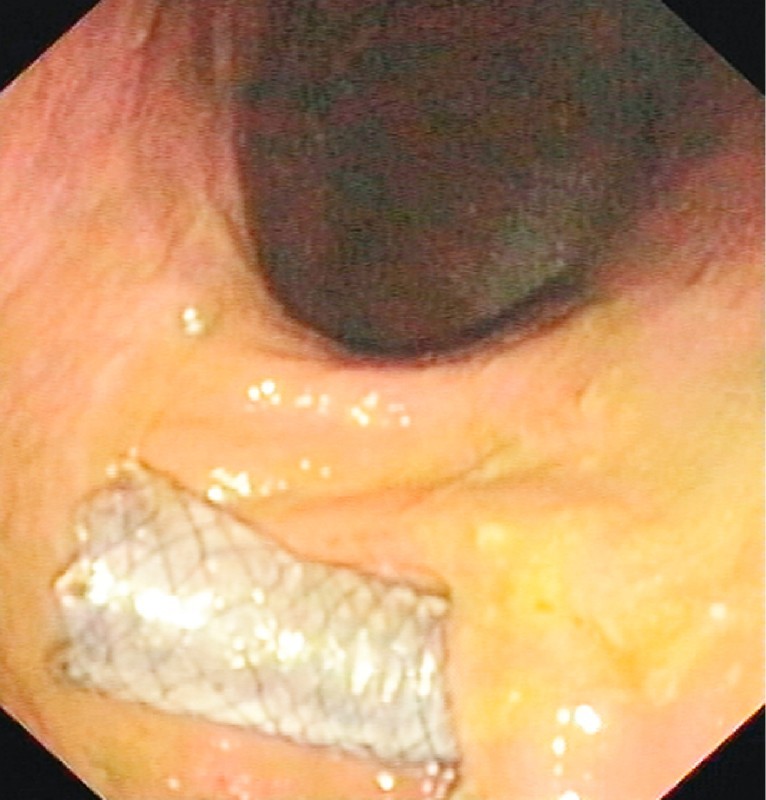
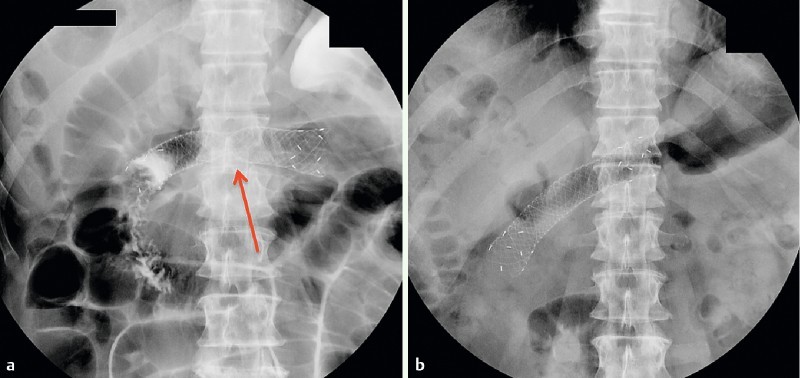
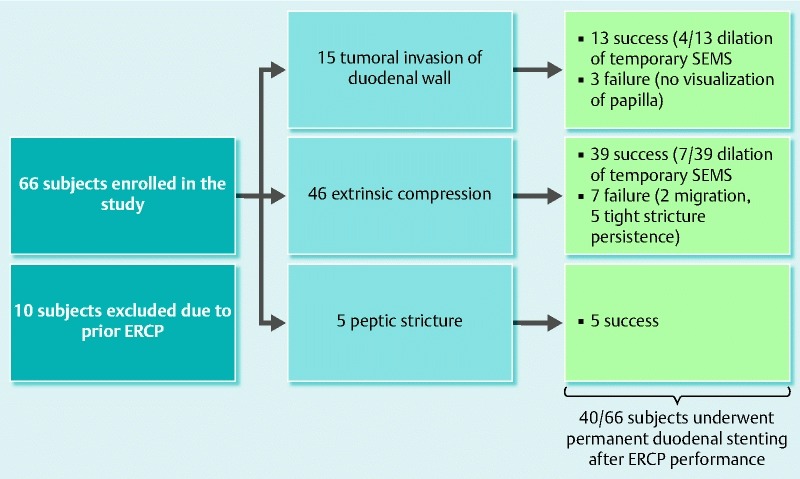
This retrospective study included 66 consecutive patients presenting with a duodenal stricture impeding the ability to perform an ERCP. Provisional duodenal stenting was performed as a bridge to ERCP. A second endoscopic session was performed to remove the provisional stent and to perform an ERCP. Afterward, a permanent duodenal stent was delivered if necessary.
Sixty-six duodenal stents (17 pcSEMS and 49 fcSEMS) were delivered with a median indwelling time of 3.15 (1 - 7) days. Two migrations occurred in the pcSEMS group, 1 of which required lower endoscopy for retrieval. No other procedure-related complications were observed. At second endoscopy a successful ERCP was performed in 56 patients (85 %); 10 patients (15 %) with endoscopic failure underwent PTBD or EUS-BD. Forty patients needed permanent duodenal stenting.
Provisional removable covered duodenal stenting as a bridge to ERCP for duodenal obstruction is safe procedure and in most cases allows successful performance of therapeutic ERCP. This technique could be a sound option as a step up approach before referring such cases for more complex techniques such as EUS-BD or PTBD.
十二指肠梗阻可能会妨碍内镜逆行胰胆管造影(ERCP)的实施。经皮经肝胆道引流(PTBD)或内镜超声引导下胆道通路建立(EUS-BD)是替代治疗方法,但它们的发病率和死亡率较高。本研究的目的是报告在因十二指肠狭窄导致乳头难以到达的情况下,使用临时全覆膜或部分覆膜自膨式十二指肠支架(pc/fcSEMS)作为ERCP桥梁的总体技术成功率和临床结果。
这项回顾性研究纳入了66例连续出现十二指肠狭窄且妨碍ERCP实施的患者。进行临时十二指肠支架置入作为ERCP的桥梁。进行第二次内镜检查以取出临时支架并实施ERCP。必要时随后置入永久性十二指肠支架。
共置入66个十二指肠支架(17个pcSEMS和49个fcSEMS),中位留置时间为3.15(1 - 7)天。pcSEMS组发生2例移位,其中1例需要通过下消化道内镜取出。未观察到其他与操作相关的并发症。在第二次内镜检查时,56例患者(85%)成功进行了ERCP;10例(15%)内镜检查失败的患者接受了PTBD或EUS-BD。40例患者需要置入永久性十二指肠支架。
对于十二指肠梗阻,使用临时可移除覆膜十二指肠支架作为ERCP的桥梁是一种安全的操作,并且在大多数情况下能够成功实施治疗性ERCP。在将此类病例转诊至更复杂的技术(如EUS-BD或PTBD)之前,作为一种逐步升级的方法,该技术可能是一个合理的选择。