Rabinowich Liane, Wendon Julia, Bernal William, Shibolet Oren
Liane Rabinowich, Oren Shibolet, Liver Unit, Department of Gastroenterology, Tel-Aviv Medical Center and Tel-Aviv University, Tel-Aviv 64239, Israel.
World J Gastroenterol. 2016 Sep 7;22(33):7595-603. doi: 10.3748/wjg.v22.i33.7595.
To assess the practice of caring for acute liver failure (ALF) patients in varying geographic locations and medical centers.
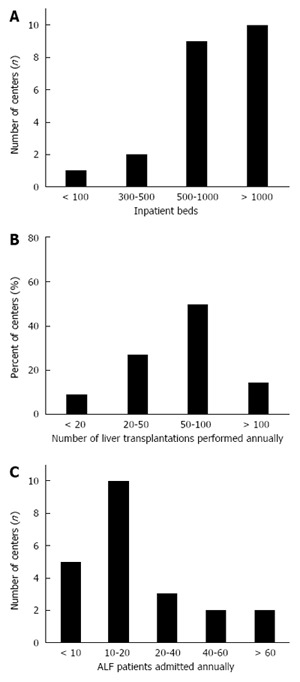
Members of the European Acute Liver Failure Consortium completed an 88-item questionnaire detailing management of ALF. Responses from 22 transplantation centers in 11 countries were analyzed, treating between 300 and 500 ALF cases and performing over 100 liver transplants (LT) for ALF annually. The questions pertained to details of the institution and their clinical activity, standards of care, referral and admission, ward- based care versus intensive care unit (ICU) as well as questions regarding liver transplantation - including criteria, limitations, and perceived performance. Clinical data was also collected from 13 centres over a 3 mo period.
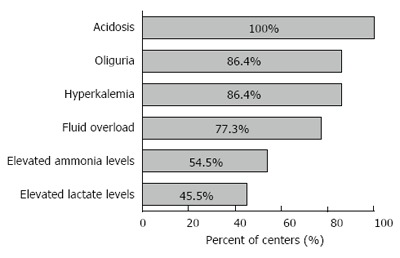
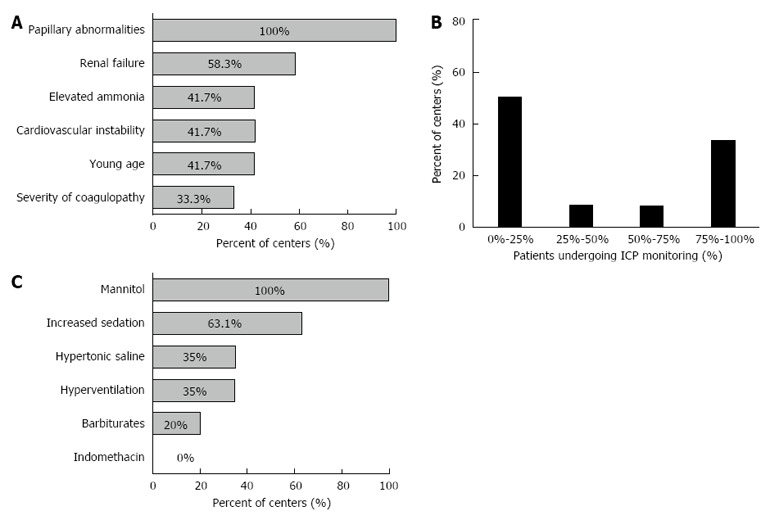
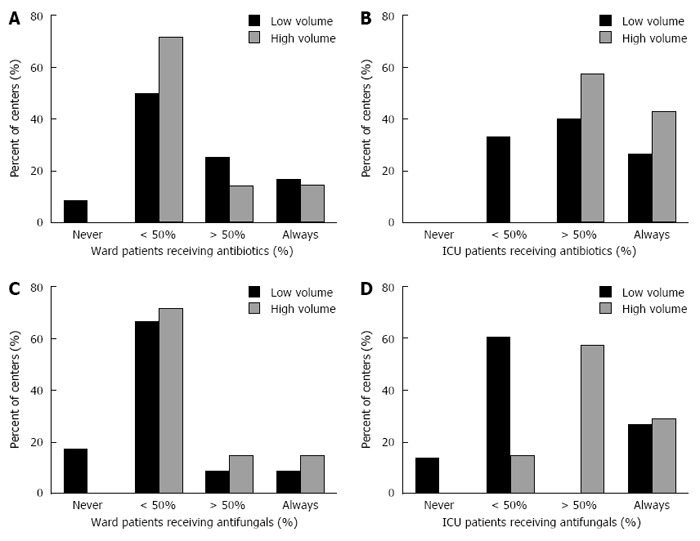
The interval between referral and admission of ALF patients to specialized units was usually less than 24 h and once admitted, treatment was provided by a multidisciplinary team. Principles of care of patients with ALF were similar among centers, particularly in relation to recognition of severity and care of the more critically ill. Centers exhibited similarities in thresholds for ICU admission and management of severe hepatic encephalopathy. Over 80% of centers administered n-acetyl-cysteine to ICU patients for non-paracetamol-related ALF. There was significant divergence in the use of prophylactic antibiotics and anti-fungals, lactulose, nutritional support and imaging investigations in admitted patients and in the monitoring and treatment of intra-cranial pressure (ICP). ICP monitoring was employed in 12 centers, with the most common indications being papilledema and renal failure. Most patients listed for transplantation underwent surgery within an average waiting time of 1-2 d. Over a period of 3 mo clinical data from 85 ALF patients was collected. Overall patient survival at 90-d was 76%. Thirty six percent of patients underwent emergency LT, with a 90% post transplant survival to hospital discharge, 42% survived with medical management alone.
Alongside similarities in principles of care of ALF patients, major areas of divergence were present in key areas of diagnosis, monitoring, treatment and decision to transplant.
评估不同地理位置和医疗中心对急性肝衰竭(ALF)患者的护理实践。
欧洲急性肝衰竭联盟成员完成了一份包含88个条目的问卷,详细描述了ALF的管理情况。分析了来自11个国家22个移植中心的回复,这些中心每年治疗300至500例ALF病例,并进行超过100例ALF肝移植(LT)。问题涉及机构详情及其临床活动、护理标准、转诊与入院、病房护理与重症监护病房(ICU),以及有关肝移植的问题,包括标准、限制和感知表现。还在3个月期间从13个中心收集了临床数据。
ALF患者转诊至专科单位与入院之间的间隔通常少于24小时,入院后由多学科团队提供治疗。各中心对ALF患者的护理原则相似,尤其是在严重程度的识别和对病情更危重患者的护理方面。各中心在ICU入院阈值和严重肝性脑病的管理方面表现出相似性。超过80%的中心对ICU中因非对乙酰氨基酚相关ALF的患者使用N - 乙酰半胱氨酸。在入院患者中预防性使用抗生素和抗真菌药物、乳果糖、营养支持和影像学检查以及颅内压(ICP)的监测和治疗方面存在显著差异。12个中心采用了ICP监测,最常见的指征是视乳头水肿和肾衰竭。大多数列入移植名单的患者在平均1 - 2天的等待时间内接受了手术。在3个月期间收集了85例ALF患者的临床数据。90天时患者总体生存率为76%。36%的患者接受了急诊LT,移植后90%存活至出院,42%仅通过药物治疗存活。
除了ALF患者护理原则存在相似性外,在诊断、监测、治疗和移植决策的关键领域存在主要差异。