Liu Liehua, Liang Yong, Zhang Hong, Wang Haoming, Guo Congtao, Pu Xiaobing, Zhang Chengmin, Wang Liyuan, Wang Jian, Lv Yingwen, Ren Zhoukui, Zhou Qiang, Deng Zhongliang
Department of Orthopedics, Chongqing No. 13 People's Hospital, Chongqing, China.
Department of Orthopedics, Orthopedics Center of PLA, Southwest Hospital, Third Military Medical University, Chongqing, China.
PLoS One. 2016 Sep 29;11(9):e0163452. doi: 10.1371/journal.pone.0163452. eCollection 2016.
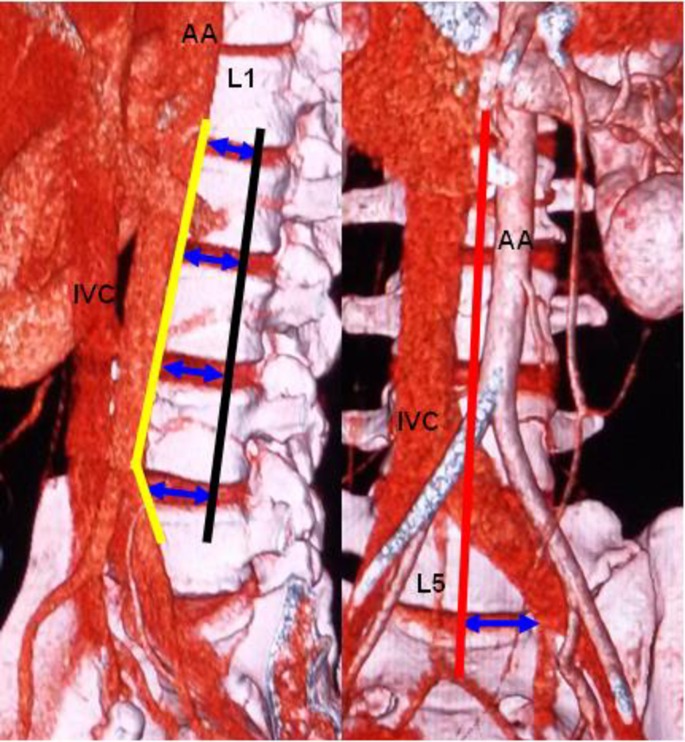
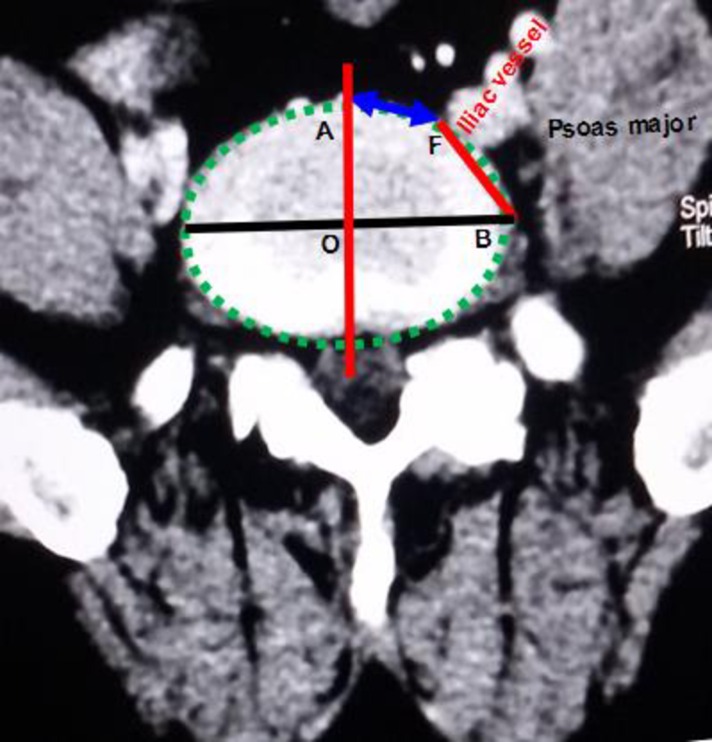
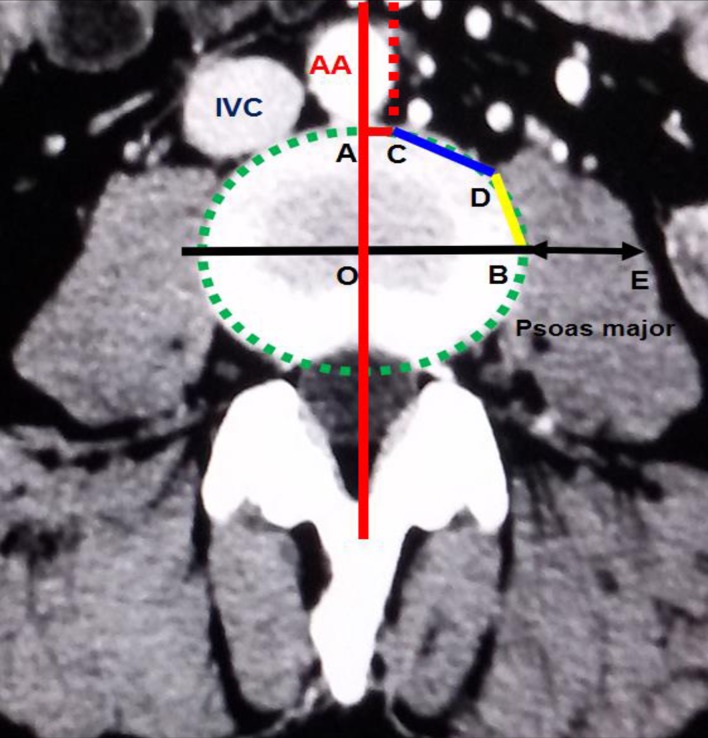
To provide applied anatomical evidence of the preoperative assessment of oblique lumbar interbody fusion (OLIF), the anatomical parameters of the OLIF operative window were observed through computed tomography angiography (CTA). We selected imaging data from 60 adults (30 males, 30 females) who underwent abdominal CTA and T12-S1 vertebral computed tomography (CT) with three-dimensional reconstruction. The OLIF operative windows at the L1-2, L2-3, L3-4, L4-5 and L5-S1 levels were as follows: the vascular window, bare window, psoas major window, ideal operative window, and actual operative window. Each level's actual operative window was statistically analyzed based on an actual operative window of <1 cm and ≥1 cm. The vascular window was largest at L4-5 (1.72 ± 0.58 cm). The bare window was largest at L5-S1 (1.59 ± 0.93 cm) and smallest at L3-4 (1.37 ± 0.51 cm). The psoas major window was largest at L3-4 (1.14 ± 0.35 cm) and smallest at L1-2 (0.41 ± 0.34 cm). The ideal operative window was largest at L4-5 (3.74 ± 0.36 cm) and smallest at L1-2 (3.23 ± 0.30 cm). The actual operative window was largest at L3-4, followed by L2-3, L4-5, L1-2, and L5-S1, which were 2.51 ± 0.56 cm, 2.28 ± 0.54 cm, 2.01 ± 0.74 cm, 1.80 ± 0.45 cm and 1.59 ± 0.93 cm, respectively (P = 0.000), and the percentages of the actual surgical window were 69%, 66%, 53%, 56% and 43%, respectively. The actual surgical window was <1 cm in 2 cases at L1-2 (3.3%), 4 cases at L4-5 (6.7%), and 17 cases at L5-S1 (28.3%) (11 males and 6 females). The regional anatomy of each level related to OLIF has its own peculiarities, and not all levels are suitable for OLIF. Before OLIF surgery, surgeons should analyze the imaging anatomy and select the appropriate surgical procedures.
为提供斜外侧腰椎椎间融合术(OLIF)术前评估的应用解剖学依据,通过计算机断层血管造影(CTA)观察OLIF手术窗口的解剖学参数。我们选取了60例接受腹部CTA及T12-S1椎体计算机断层扫描(CT)三维重建的成年人(男30例,女30例)的影像资料。L1-2、L2-3、L3-4、L4-5和L5-S1节段的OLIF手术窗口如下:血管窗口、裸区窗口、腰大肌窗口、理想手术窗口和实际手术窗口。根据实际手术窗口<1 cm和≥1 cm对各节段的实际手术窗口进行统计学分析。血管窗口在L4-5节段最大(1.72±0.58 cm)。裸区窗口在L5-S1节段最大(1.59±0.93 cm),在L3-4节段最小(1.37±0.51 cm)。腰大肌窗口在L3-4节段最大(1.14±0.35 cm),在L1-2节段最小(0.41±0.34 cm)。理想手术窗口在L4-5节段最大(3.74±0.36 cm),在L1-2节段最小(3.23±0.30 cm)。实际手术窗口在L3-4节段最大,其次为L2-3、L4-5、L1-2和L5-S1节段,分别为2.51±0.56 cm、2.28±0.54 cm、2.01±0.74 cm、1.80±0.45 cm和1.59±0.93 cm(P = 0.000),实际手术窗口的占比分别为69%、66%、53%、56%和43%。L1-2节段有2例(3.3%)、L4-5节段有4例(6.7%)、L5-S1节段有17例(28.3%)(男11例,女6例)的实际手术窗口<1 cm。与OLIF相关的各节段区域解剖各有特点,并非所有节段都适合OLIF。在OLIF手术前,外科医生应分析影像解剖结构并选择合适的手术方式。