DeBoer Mark D, Scharf Rebecca J, Leite Alvaro M, Férrer Alessandra, Havt Alexandre, Pinkerton Relana, Lima Aldo A, Guerrant Richard L
Pediatric Endocrinology, Department of Pediatrics, University of Virginia, Charlottesville, VA.
Developmental Pediatrics, Department of Pediatrics, University of Virginia, Charlottesville, VA.
Nutrition. 2017 Jan;33:248-253. doi: 10.1016/j.nut.2016.06.013. Epub 2016 Jul 26.
Deficits in weight gain and linear growth are seen frequently among children in areas where malnutrition and recurrent infections are common. Although both inflammation and malnutrition can result in growth hormone (GH) resistance, the interrelationships of infection, inflammation, and growth deficits in developing areas remain unclear. The aim of this study was to evaluate relationships between low levels of systemic inflammation, growth factors, and anthropometry in a case-control cohort of underweight and normal weight children in northern Brazil.
We evaluated data from 147 children ages 6 to 24 mo evaluated in the MAL-ED (Interactions of Malnutrition and Enteric Disease) case-control study following recruitment from a nutrition clinic for impoverished families in Fortaleza, Brazil. We used nonparametric tests and linear regression to evaluate relationships between current symptoms of infections (assessed by questionnaire), systemic inflammation (assessed by high-sensitivity C-reactive protein [hsCRP]), the GH insulin-like growth factor-1 (IGF-1) axis, and measures of anthropometry. All models were adjusted for age and sex.
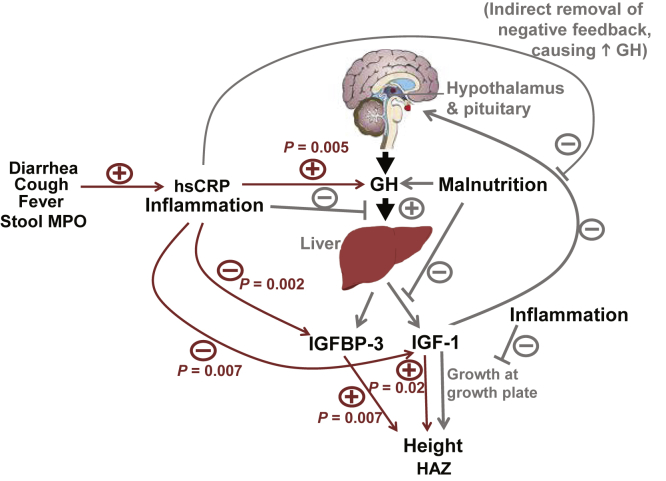
Children with recent symptoms of diarrhea, cough, and fever (compared with those without symptoms) had higher hsCRP levels; those with recent diarrhea and fever also had lower IGF-1 and higher GH levels. Stool myeloperoxidase was positively associated with serum hsCRP. hsCRP was in turn positively associated with GH and negatively associated with IGF-1 and IGF-binding protein-3 (IGFBP-3), suggesting a state of GH resistance. After adjustment for hsCRP, IGF-1 and IGFBP-3 were positively and GH was negatively associated with Z scores for height and weight.
Infection and inflammation were linked to evidence of GH resistance, whereas levels of GH, IGF-1, and IGFBP-3 were associated with growth indices independent of hsCRP. These data implicate complex interrelationships between infection, nutritional status, GH axis, and linear growth in children from a developing area.
在营养不良和反复感染常见的地区,儿童体重增加和线性生长不足的情况屡见不鲜。尽管炎症和营养不良均可导致生长激素(GH)抵抗,但在发展中地区,感染、炎症与生长不足之间的相互关系仍不明确。本研究旨在评估巴西北部体重过轻和体重正常儿童的病例对照队列中,全身炎症水平低、生长因子与人体测量学之间的关系。
我们评估了147名6至24个月大儿童的数据,这些儿童是在巴西福塔莱萨一家为贫困家庭开设的营养诊所招募后,参与MAL-ED(营养不良与肠道疾病的相互作用)病例对照研究的。我们使用非参数检验和线性回归来评估感染的当前症状(通过问卷评估)、全身炎症(通过高敏C反应蛋白[hsCRP]评估)、GH胰岛素样生长因子-1(IGF-1)轴与人体测量学指标之间的关系。所有模型均根据年龄和性别进行了调整。
近期有腹泻、咳嗽和发热症状的儿童(与无症状儿童相比)hsCRP水平较高;近期有腹泻和发热症状的儿童IGF-1水平也较低,GH水平较高。粪便髓过氧化物酶与血清hsCRP呈正相关。hsCRP又与GH呈正相关,与IGF-1和胰岛素样生长因子结合蛋白-3(IGFBP-3)呈负相关,提示存在GH抵抗状态。在对hsCRP进行调整后,IGF-1和IGFBP-3与身高和体重的Z评分呈正相关,GH与身高和体重的Z评分呈负相关。
感染和炎症与GH抵抗的证据相关,而GH、IGF-1和IGFBP-3的水平与独立于hsCRP的生长指数相关。这些数据表明,发展中地区儿童的感染、营养状况、GH轴和线性生长之间存在复杂的相互关系。