Aubron Cécile, DePuydt Joris, Belon François, Bailey Michael, Schmidt Matthieu, Sheldrake Jayne, Murphy Deirdre, Scheinkestel Carlos, Cooper D Jamie, Capellier Gilles, Pellegrino Vincent, Pilcher David, McQuilten Zoe
The Australian and New Zealand Intensive Care Research Centre, Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Australia.
The Transfusion Research Unit, Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Australia.
Ann Intensive Care. 2016 Dec;6(1):97. doi: 10.1186/s13613-016-0196-7. Epub 2016 Oct 6.
Bleeding is the most frequent complication associated with extracorporeal membrane oxygenation (ECMO) support in critically ill patients. Nonetheless, risk factors for bleeding have been poorly described especially those associated with coagulation anomalies and anticoagulant therapy during ECMO support. The aim of this study is to describe bleeding complications in critically ill patients undergoing ECMO and to identify risk factors for bleeding events.
We retrospectively analysed ICU charts of adults who received either veno-venous (VV) or veno-arterial (VA) ECMO support in two participating ICUs between 2010 and 2013. Characteristics of patients with and without bleeding complications, as per the Extracorporeal Life Support Organisation (ELSO) definition, were compared, and the impact of bleeding complications on patient outcomes was assessed using survival analysis. Variables that were independently associated with bleeding, including daily clinical and biological variables during ECMO courses, were modelled.
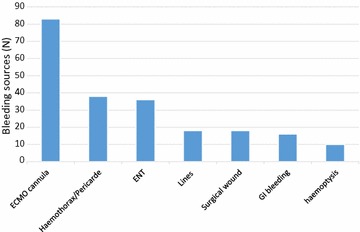
Of the 149 ECMO episodes (111 VA ECMO and 38 VV ECMO) performed in 147 adults, 89 episodes (60 %) were complicated by at least one bleeding event. The most common bleeding sources were: ECMO cannula (37 %), haemothorax or cardiac tamponade (17 %) and ear-nose and throat (16 %). Intra-cranial haemorrhage occurred in five (2.2 %) patients. Bleeding complications were independently associated with worse survival [adjusted hazard ratio (HR) 2.17, 95 % confidence interval (CI) 1.07-4.41, P = 0.03]. Higher activated partial thromboplastin time (aPTT) [adjusted odds ratio (OR) 3.00, 95 % CI 1.64-5.47, P < 0.01], APACHE III score [adjusted OR 1.01, 95 % CI 1.01-1.02, P = 0.01] and ECMO following surgery [adjusted OR 3.04, 95 % CI 1.62-5.69, P < 0.01] were independently associated with greater risk of bleeding occurrence. A similar association between bleeding and higher aPTT was found when non-post-surgical VA ECMO was considered separately.
Bleeding events based on the ELSO bleeding definition occurred in more than 60 % of ECMO episodes and were associated with hospital mortality. We identified higher aPTT prior bleeding as an independent risk factor for bleeding event, suggesting that better control of the aPTT (through a better control of either coagulopathy or anticoagulation) may improve patients' outcome.
出血是危重症患者体外膜肺氧合(ECMO)支持治疗中最常见的并发症。然而,出血的危险因素,尤其是与ECMO支持期间凝血异常和抗凝治疗相关的危险因素,一直鲜有描述。本研究旨在描述接受ECMO治疗的危重症患者的出血并发症,并确定出血事件的危险因素。
我们回顾性分析了2010年至2013年间在两个参与研究的重症监护病房接受静脉-静脉(VV)或静脉-动脉(VA)ECMO支持的成年患者的重症监护病房病历。比较了符合体外生命支持组织(ELSO)定义的有出血并发症和无出血并发症患者的特征,并使用生存分析评估出血并发症对患者预后的影响。对与出血独立相关的变量进行建模,包括ECMO治疗期间的每日临床和生物学变量。
在147名成年人中进行的149次ECMO治疗(111次VA ECMO和38次VV ECMO)中,89次治疗(60%)至少发生了一次出血事件。最常见的出血部位是:ECMO插管(37%)、血胸或心脏压塞(17%)以及耳鼻喉(16%)。5名(2.2%)患者发生了颅内出血。出血并发症与较差的生存率独立相关[调整后的风险比(HR)为2.17,95%置信区间(CI)为1.07-4.41,P = 0.03]。较高的活化部分凝血活酶时间(aPTT)[调整后的优势比(OR)为3.00,95%CI为1.64-5.47,P < 0.01]、急性生理与慢性健康状况评分系统III(APACHE III)评分[调整后的OR为1.01,95%CI为1.01-1.02,P = 0.01]以及手术后进行ECMO治疗[调整后的OR为3.04,95%CI为1.62-5.69,P < 0.01]与出血发生风险增加独立相关。当单独考虑非手术后的VA ECMO时,也发现出血与较高的aPTT之间存在类似关联。
根据ELSO出血定义,超过60%的ECMO治疗发生了出血事件,且与医院死亡率相关。我们确定出血前较高的aPTT是出血事件的独立危险因素,这表明更好地控制aPTT(通过更好地控制凝血障碍或抗凝)可能改善患者的预后。