Nielsen Vibe Maria Laden, Madsen Jacob, Aasen Anette, Toft-Petersen Anne Pernille, Lübcke Kenneth, Rasmussen Bodil Steen, Christensen Erika Frischknecht
Department of Anaesthesiology and Intensive Care Medicine, Aalborg University Hospital, Aalborg, Denmark.
Department of Clinical Medicine, Aalborg University, Aalborg, Denmark.
Scand J Trauma Resusc Emerg Med. 2016 Oct 10;24(1):121. doi: 10.1186/s13049-016-0315-3.
Patients with acute respiratory failure are at risk of deterioration during prehospital transport. Ventilatory support with continuous positive airway pressure (CPAP) can be initiated in the prehospital setting. The objective of the study is to evaluate adherence to treatment and effectiveness of CPAP as an addition to standard care.
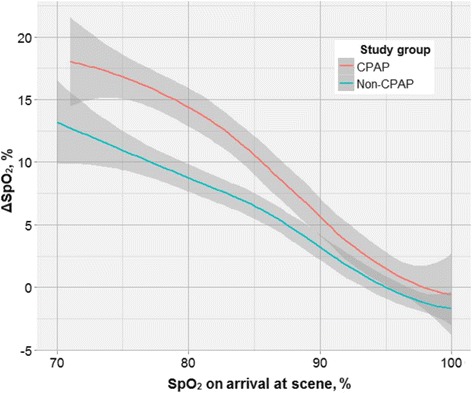
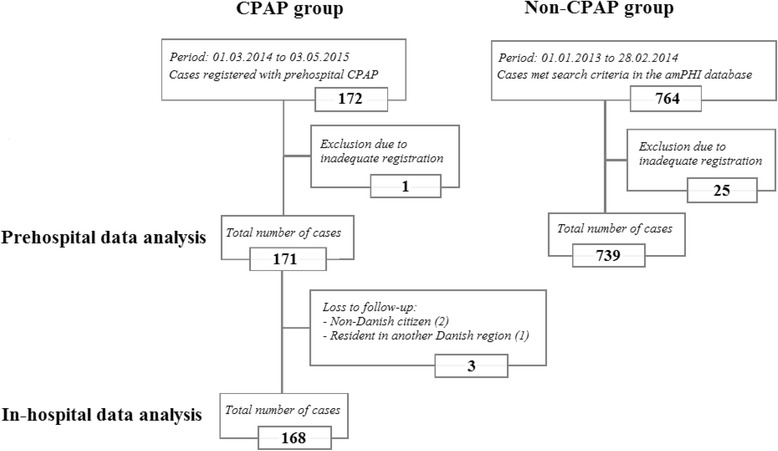
In North Denmark Region, patients with acute respiratory failure, whom paramedics assessed as suffering from acute cardiopulmonary oedema, acute exacerbation of chronic obstructive pulmonary disease or asthma were treated with CPAP using 100 % O from 1 March 2014 to 3 May 2015. Adherence to treatment was evaluated by number of adverse events and discontinuation of treatment. Intensive care admissions and mortality were reported in this cohort. Effectiveness was evaluated by changes in peripheral oxygen saturation (SpO) and respiratory rate during transport and compared to a historical control (non-CPAP) group treated with standard care only. Values were compared by hypothesis testing and linear modelling of SpO on arrival at scene and ΔSpO stratified according to treatment group.
In fourteen months, 171 patients were treated with CPAP (mean treatment time 35 ± 18 min). Adverse events were reported in 15 patients (9 %), hereof six discontinued CPAP due to hypotension, nausea or worsening dyspnoea. One serious adverse event was reported, a suspected pneumothorax treated adequately by an anaesthesiologist called from a mobile emergency care unit. Among CPAP patients, 45 (27 %) were admitted to an intensive care unit and 24 (14 %) died before hospital discharge. The non-CPAP group consisted of 739 patients. From arrival at scene to arrival at hospital, CPAP patients had a larger increase in SpO than non-CPAP patients (87 to 96 % versus 92 to 96 %, p < 0.01) and a larger decrease in respiratory rate (32 to 25 versus 28 to 24 breaths/min, p < 0.01). In a linear model, CPAP was superior to non-CPAP in patients with initial SpO ≤90 % (p < 0.05). One CPAP patient (0.6 %) and eight non-CPAP patients (1.1 %) were intubated in the prehospital setting.
The study design reflects the daily prehospital working environment including long transport timesand paramedics educated in treating symptoms of acute respiratory failure, rather than treating one specific diagnosis. The study population was included consecutively and few patients were lost to follow-up. However, the study was too small to allow assessment of any effect of prehospital CPAP on mortality, nor could the effectiveness in specific disease conditions be examined.
In an emergency medical service including physician backup, adherence to CPAP treatment administered by paramedics was high and treatment was effective in patients with acute respiratory failure.
急性呼吸衰竭患者在院前转运过程中存在病情恶化风险。可在院前环境中启动持续气道正压通气(CPAP)进行通气支持。本研究的目的是评估对治疗的依从性以及CPAP作为标准治疗补充措施的有效性。
在丹麦北部地区,2014年3月1日至2015年5月3日期间,护理人员评估为患有急性心源性肺水肿、慢性阻塞性肺疾病急性加重或哮喘的急性呼吸衰竭患者接受了使用100%氧气的CPAP治疗。通过不良事件数量和治疗中断情况评估对治疗的依从性。报告了该队列中的重症监护病房收治情况和死亡率。通过转运期间外周血氧饱和度(SpO)和呼吸频率的变化评估有效性,并与仅接受标准治疗的历史对照组(非CPAP组)进行比较。通过假设检验和到达现场时SpO的线性建模以及根据治疗组分层的ΔSpO对数值进行比较。
在14个月内,171例患者接受了CPAP治疗(平均治疗时间35±18分钟)。15例患者(9%)报告了不良事件,其中6例因低血压、恶心或呼吸困难加重而停用CPAP。报告了1例严重不良事件,一名从移动急救单元叫来的麻醉医生对疑似气胸进行了妥善处理。在CPAP患者中,45例(27%)被收治入重症监护病房,24例(14%)在出院前死亡。非CPAP组由739例患者组成。从到达现场到到达医院,CPAP患者的SpO升高幅度大于非CPAP患者(87%至96%对92%至96%,p<0.01),呼吸频率下降幅度更大(32次/分钟至25次/分钟对28次/分钟至24次/分钟,p<0.01)。在一个线性模型中,初始SpO≤90%的患者中,CPAP优于非CPAP(p<0.05)。1例CPAP患者(0.6%)和8例非CPAP患者(1.1%)在院前环境中接受了插管。
本研究设计反映了日常院前工作环境,包括较长的转运时间以及接受过急性呼吸衰竭症状治疗培训的护理人员,而非针对某一特定诊断进行治疗。研究人群是连续纳入的,很少有患者失访。然而,该研究规模太小,无法评估院前CPAP对死亡率的任何影响,也无法检查特定疾病状况下的有效性。
在包括医生后备支持的紧急医疗服务中,护理人员对CPAP治疗的依从性较高,且CPAP治疗对急性呼吸衰竭患者有效。