Department of Hematology and Oncology, University Hospital Halle, Halle/Saale, Germany.
PLoS One. 2016 Oct 12;11(10):e0164587. doi: 10.1371/journal.pone.0164587. eCollection 2016.
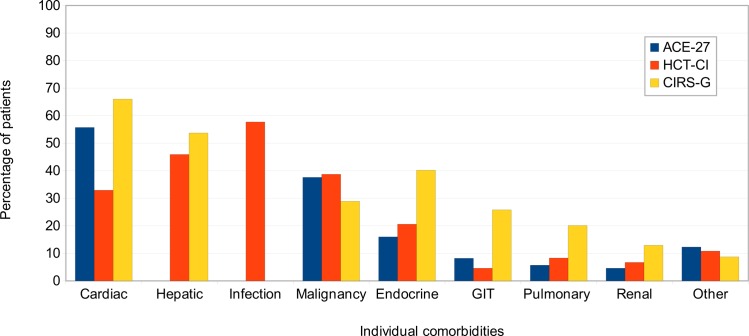
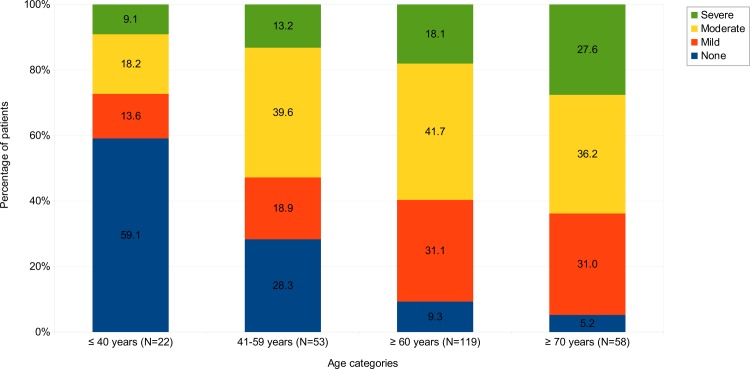
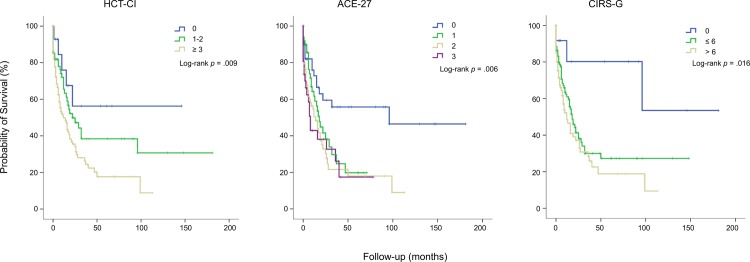
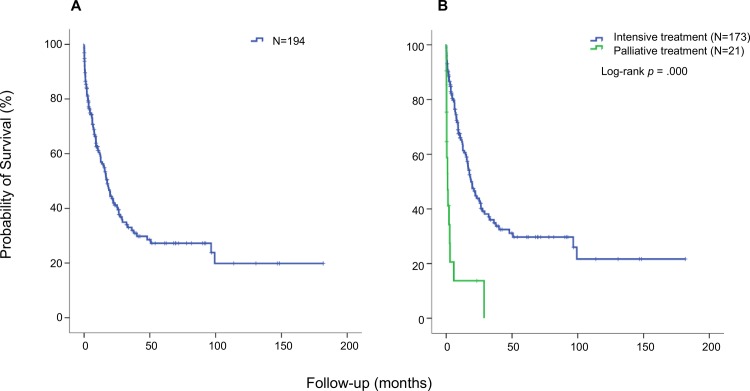
Age is a dominant predictor of outcome in acute myeloid leukemia (AML). However, it is not clear to which extent comorbidities contribute to this effect. The objective of this study was to determine the impact of pretreatment comorbidities on survival of AML patients. In a single-center retrospective study 194 adult AML patients were included. The Hematopoietic cell transplantation comorbidity index (HCT-CI), the Adult Comorbidity Evaluation-27 (ACE-27) score and the Cumulative Illness Rating Scale for Geriatrics (CIRS-G) as well as data on demographics, cytogenetics, treatment and outcome were evaluated at the time of initial diagnosis by univariate and multivariate analysis. The study included 102 male and 92 female (median age 60.9 years) of which 173 (89.2%) received intensive chemotherapy. Median overall survival (OS) was 17 months. In univariate analysis, cardiovascular disease (26 vs 12 months, p = .005), severe hepatic disease (19 vs 4 months, p = .013) and renal impairment (17 vs 7 months, p = .016) was associated with inferior OS. For each index, the highest comorbidity burden was associated with reduced OS. However, in multivariate analysis only the ACE-27 score was associated with outcome. Besides ECOG ≥ 2 and poor cytogenetics only the ACE-27 score but not higher age was associated with OS in the group of patients receiving intensive therapy. Adjusted hazard ratios were 3.1, 3.5 and 4.0 for mild, moderate and severe ACE-27-assessed comorbidities, respectively (p = .012). Our study confirms that comorbidities significantly impact survival of AML patients and a pretreatment assessment of comorbidities may help to identify patients with poor outcome.
年龄是急性髓系白血病(AML)预后的主要预测因素。然而,尚不清楚合并症在多大程度上影响这一结果。本研究旨在确定预处理合并症对 AML 患者生存的影响。在一项单中心回顾性研究中,纳入了 194 例成人 AML 患者。在初始诊断时,通过单因素和多因素分析评估了造血细胞移植合并症指数(HCT-CI)、成人合并症评估-27 评分(ACE-27)、老年累积疾病评分量表(CIRS-G)以及人口统计学、细胞遗传学、治疗和预后数据。该研究包括 102 名男性和 92 名女性(中位年龄 60.9 岁),其中 173 名(89.2%)接受了强化化疗。中位总生存期(OS)为 17 个月。单因素分析显示,心血管疾病(26 个月 vs 12 个月,p =.005)、严重肝脏疾病(19 个月 vs 4 个月,p =.013)和肾功能不全(17 个月 vs 7 个月,p =.016)与 OS 降低相关。对于每个指标,合并症负担最高与 OS 降低相关。然而,多因素分析仅 ACE-27 评分与预后相关。除 ECOG ≥ 2 和不良细胞遗传学外,仅 ACE-27 评分而非更高年龄与接受强化治疗的患者的 OS 相关。轻度、中度和重度 ACE-27 评估的合并症的调整后的危险比分别为 3.1、3.5 和 4.0(p =.012)。本研究证实,合并症显著影响 AML 患者的生存,预处理合并症评估可能有助于识别预后不良的患者。