Kumar Abhyuday, Seth Anita, Prakash Smita, Deganwa Mangilal, Gogia Anoop Raj
Department of Anaesthesia and Critical Care, All India Institute of Medical Sciences, New Delhi, India.
Department of Anaesthesia and Intensive Care, Vardhman Mahavir Medical College and Safdarjang Hospital, New Delhi, India.
Anesth Essays Res. 2016 Sep-Dec;10(3):661-666. doi: 10.4103/0259-1162.191113.
The present study was undertaken to compare and evaluate the efficacy of intravenous (IV) fentanyl and lignocaine airway nebulization and a combination of both in attenuating the hemodynamic response to laryngoscopy and tracheal intubation.
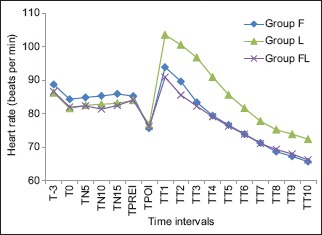
Ninety-six patients of either sex aged between 18 and 65 years of age, belonging to the American Society of Anesthesiologists (ASA) health status Classes I and II, undergoing elective surgery requiring general anesthesia with endotracheal intubation were included in the study. Patients were randomly divided into three groups. Group F received IV fentanyl 2 μg/kg, Group L received nebulization with 3 mg/kg of 4% lignocaine, and Group FL received both nebulization with 3 mg/kg of 4% lignocaine and IV fentanyl 2 μg/kg before intubation. Hemodynamic parameters were noted before and immediately after induction, 1 min after intubation, and every minute after intubation for 10 min.
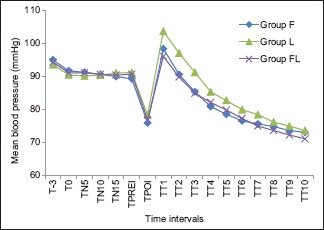
Hemodynamic response to laryngoscopy and intubation was not completely abolished in any of the groups. Nebulized lignocaine was least effective in attenuating hemodynamic response to intubation, and hemodynamic parameters were significantly high after intubation as compared to other groups. Fentanyl alone or in combination with nebulized lignocaine was most effective, and Group F and Group FL were comparable. The maximum increase in mean blood pressure after intubation from baseline in Groups F, L, and FL was 7.4%, 14.6%, and 5.4%, respectively.
In our study, IV fentanyl 2 μg/kg administered 5 min before induction was found to be the most effective in attenuating the hemodynamic response. There was no advantage to the use of nebulized lignocaine in attenuating the hemodynamic response to laryngoscopy and intubation.
本研究旨在比较和评估静脉注射芬太尼和利多卡因气道雾化以及两者联合使用在减轻喉镜检查和气管插管引起的血流动力学反应方面的疗效。
纳入96例年龄在18至65岁之间、属于美国麻醉医师协会(ASA)健康状况I级和II级、接受需要全身麻醉和气管插管的择期手术的患者。患者被随机分为三组。F组静脉注射2μg/kg芬太尼,L组雾化吸入3mg/kg的4%利多卡因,FL组在插管前既雾化吸入3mg/kg的4%利多卡因又静脉注射2μg/kg芬太尼。记录诱导前、诱导后即刻、插管后1分钟以及插管后10分钟内每分钟的血流动力学参数。
在任何一组中,喉镜检查和插管引起的血流动力学反应均未完全消除。雾化利多卡因在减轻插管引起的血流动力学反应方面效果最差,与其他组相比,插管后的血流动力学参数明显较高。单独使用芬太尼或与雾化利多卡因联合使用最有效,F组和FL组相当。F组、L组和FL组插管后平均血压相对于基线的最大升高分别为7.4%、14.6%和5.4%。
在我们的研究中,发现诱导前5分钟静脉注射2μg/kg芬太尼在减轻血流动力学反应方面最有效。在减轻喉镜检查和插管引起的血流动力学反应方面,使用雾化利多卡因没有优势。