Kann Inger Cathrine, Lundqvist Christofer, Lurås Hilde
Health Services Research Centre (HØKH), Akershus University Hospital, PO Box 1000, 1478, Lørenskog, Norway.
Institute of Clinical Medicine, Campus Ahus, University of Oslo, Oslo, Norway.
Drugs Real World Outcomes. 2015 Sep;2(3):193-198. doi: 10.1007/s40801-015-0036-3.
Polypharmacy, i.e. the simultaneous use of multiple drugs, is known to be associated with compliance errors and adverse drug reactions. Norway has a list-patient system in general practice, formalizing the relationship between the patient and his/her regular general practitioner (GP). One important aim with a list-patient system is to secure medical quality in primary care by giving the GP the responsibility for coordinating the medical treatment.
To examine the regular GP's role in polypharmacy to the home-dwelling elderly in Norway and to determine by how much multiple prescribers increase the risk of polypharmacy.
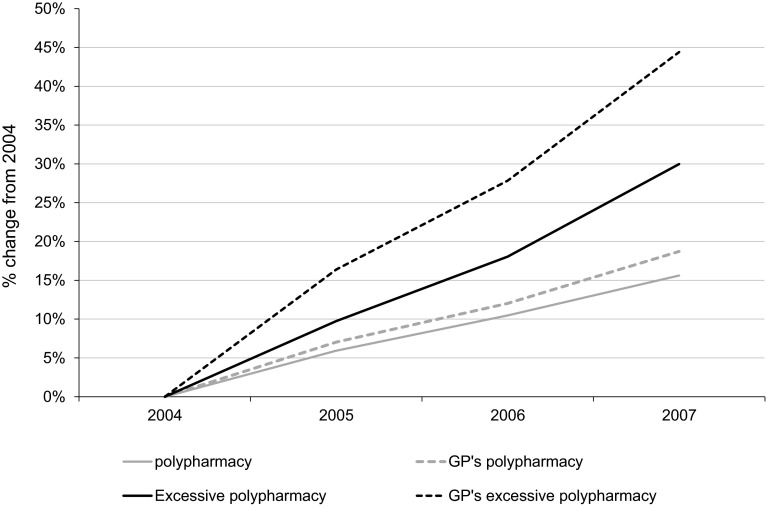
This was a population registry study based on data on all prescription drugs dispensed at pharmacies to patients 70 years and older from the Norwegian Prescription Database, merged with data on GPs and GPs' patient lists from the Regular General Practitioner Database. The dataset included 624,308 patients and 4520 GPs in the period from 2004 to 2007. Outcome measures were: number of drug-substances prescribed and dispensed per patient by the regular GP, other GPs, non-GP specialists and hospital doctors; polypharmacy, defined as five or more prescribed and dispensed substances in the same quarter; excessive polypharmacy, defined as ten or more prescribed and dispensed substances in the same quarter.
Polypharmacy is high and increasing despite the list-patient system. GPs prescribe all the substances that cause polypharmacy in 64 % of the incidents, but the patients' risk of polypharmacy increases substantially with number of prescribers, odds ratio 2.32 (95 % CI 2.31-2.33).
GPs have a major role in the high and increasing polypharmacy among the elderly in Norway. Any intervention intending to improve the situation must necessarily include the GPs.
多重用药,即同时使用多种药物,已知与用药依从性错误和药物不良反应相关。挪威在全科医疗中有患者名单系统,规范了患者与其常规全科医生(GP)之间的关系。患者名单系统的一个重要目标是通过让全科医生负责协调医疗治疗来确保初级医疗的质量。
研究挪威常规全科医生在居家老年人多重用药中的作用,并确定多个开处方者会使多重用药风险增加多少。
这是一项基于人口登记的研究,数据来源于挪威处方数据库中所有配发给70岁及以上患者的处方药,以及常规全科医生数据库中关于全科医生及其患者名单的数据。数据集包括2004年至2007年期间的624308名患者和4520名全科医生。结果指标为:常规全科医生、其他全科医生、非全科专科医生和医院医生为每位患者开具和配发的药物物质数量;多重用药,定义为同一季度内开具和配发五种或更多药物物质;过度多重用药,定义为同一季度内开具和配发十种或更多药物物质。
尽管有患者名单系统,多重用药情况仍然严重且呈上升趋势。在64%的事件中,全科医生开具了所有导致多重用药的药物物质,但患者的多重用药风险随着开处方者数量的增加而大幅上升,优势比为2.32(95%可信区间2.31 - 2.33)。
全科医生在挪威老年人中严重且不断增加的多重用药情况中起主要作用。任何旨在改善这种情况的干预措施都必须包括全科医生。