Masnoon Nashwa, Shakib Sepehr, Kalisch-Ellett Lisa, Caughey Gillian E
Quality Use of Medicines and Pharmacy Research Centre, School of Pharmacy and Medical Sciences, University of South Australia, Frome Road, Adelaide, South Australia, Australia.
Department of Pharmacy, Royal Adelaide Hospital, North Terrace, Adelaide, South Australia, Australia.
BMC Geriatr. 2017 Oct 10;17(1):230. doi: 10.1186/s12877-017-0621-2.
Multimorbidity and the associated use of multiple medicines (polypharmacy), is common in the older population. Despite this, there is no consensus definition for polypharmacy. A systematic review was conducted to identify and summarise polypharmacy definitions in existing literature.
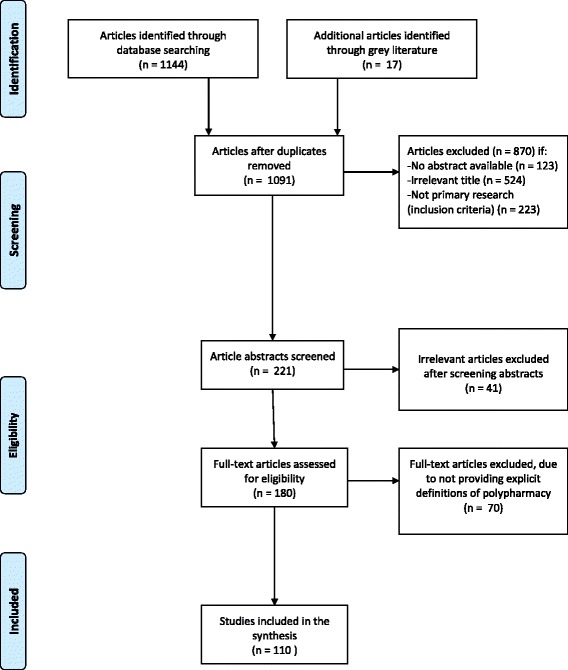
The reporting of this systematic review conforms to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) checklist. MEDLINE (Ovid), EMBASE and Cochrane were systematically searched, as well as grey literature, to identify articles which defined the term polypharmacy (without any limits on the types of definitions) and were in English, published between 1st January 2000 and 30th May 2016. Definitions were categorised as i. numerical only (using the number of medications to define polypharmacy), ii. numerical with an associated duration of therapy or healthcare setting (such as during hospital stay) or iii. Descriptive (using a brief description to define polypharmacy).
A total of 1156 articles were identified and 110 articles met the inclusion criteria. Articles not only defined polypharmacy but associated terms such as minor and major polypharmacy. As a result, a total of 138 definitions of polypharmacy and associated terms were obtained. There were 111 numerical only definitions (80.4% of all definitions), 15 numerical definitions which incorporated a duration of therapy or healthcare setting (10.9%) and 12 descriptive definitions (8.7%). The most commonly reported definition of polypharmacy was the numerical definition of five or more medications daily (n = 51, 46.4% of articles), with definitions ranging from two or more to 11 or more medicines. Only 6.4% of articles classified the distinction between appropriate and inappropriate polypharmacy, using descriptive definitions to make this distinction.
Polypharmacy definitions were variable. Numerical definitions of polypharmacy did not account for specific comorbidities present and make it difficult to assess safety and appropriateness of therapy in the clinical setting.
多种疾病并存以及相关的多种药物联用(多重用药)在老年人群中很常见。尽管如此,对于多重用药尚无共识性定义。开展了一项系统评价以识别和总结现有文献中的多重用药定义。
本系统评价的报告遵循系统评价和Meta分析的首选报告项目(PRISMA)清单。对MEDLINE(Ovid)、EMBASE和Cochrane进行了系统检索,以及灰色文献,以识别定义了多重用药术语(对定义类型无任何限制)且为英文、于2000年1月1日至2016年5月30日发表的文章。定义被分类为:i. 仅为数值型(使用药物数量来定义多重用药),ii. 数值型并伴有相关治疗持续时间或医疗环境(如住院期间),或iii. 描述性(使用简短描述来定义多重用药)。
共识别出1156篇文章,110篇文章符合纳入标准。文章不仅定义了多重用药,还定义了诸如轻度和重度多重用药等相关术语。结果,共获得了138个多重用药及相关术语的定义。有111个仅为数值型定义(占所有定义的80.4%),15个纳入了治疗持续时间或医疗环境的数值型定义(10.9%),以及12个描述性定义(8.7%)。最常报告的多重用药定义是每日使用五种或更多药物的数值型定义(n = 51,占文章的46.4%),定义范围从两种或更多到11种或更多药物。只有6.4%的文章使用描述性定义对适当和不适当多重用药进行了区分。
多重用药定义存在差异。多重用药的数值型定义未考虑存在的特定合并症,难以在临床环境中评估治疗的安全性和适当性。