Mease Philip J
Swedish Medical Center and University of Washington School of Medicine, 601 Broadway, Suite 600, Seattle, WA, 98122, USA.
Rheumatol Ther. 2014 Dec;1(1):1-20. doi: 10.1007/s40744-014-0005-4. Epub 2014 Dec 9.
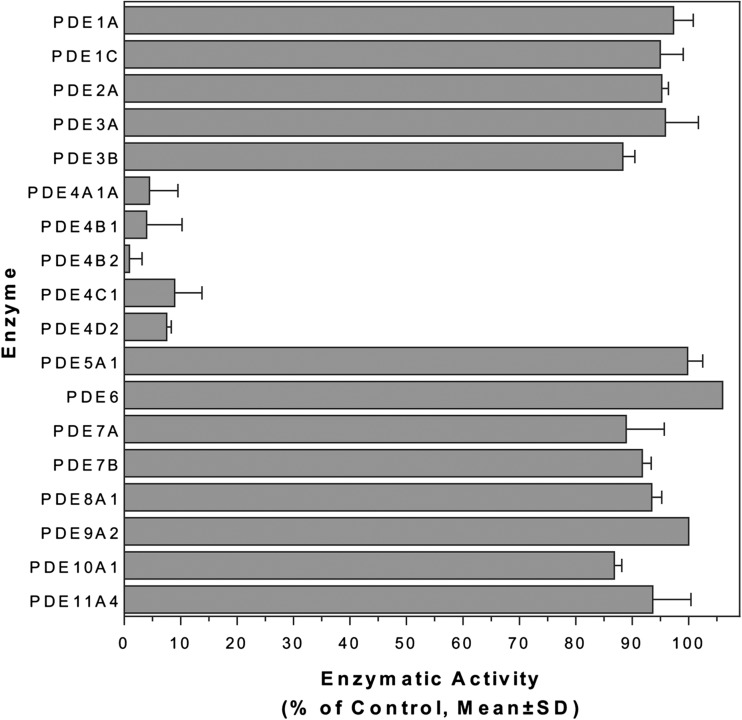
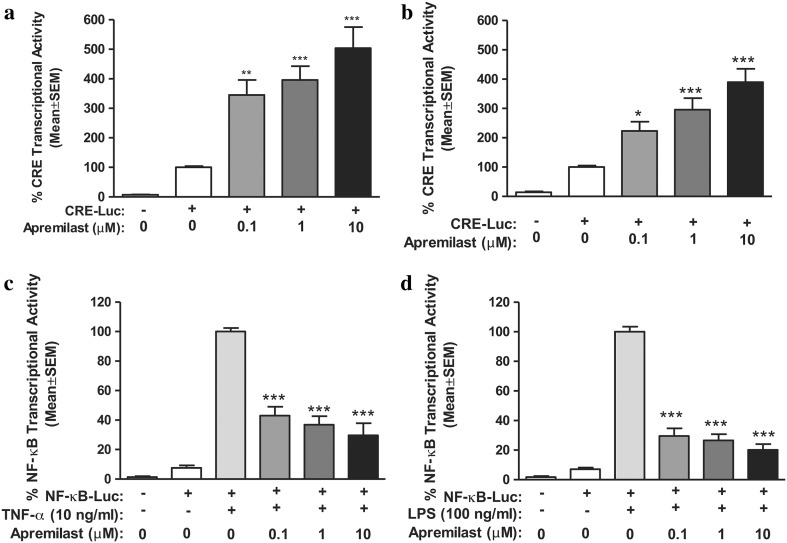
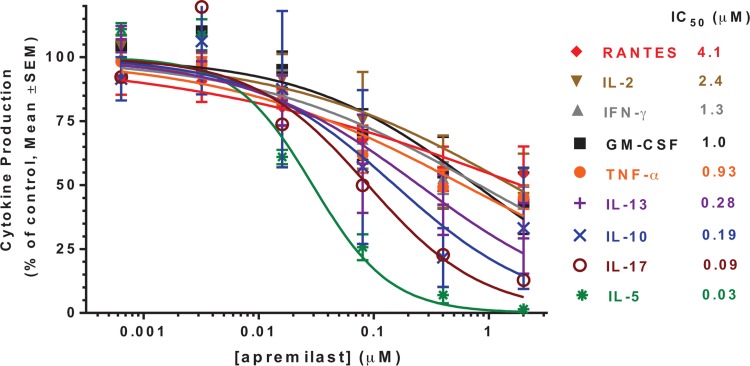
Psoriatic arthritis (PsA) is a spondyloarthritis that occurs in up to 30% of psoriasis patients. Patients with PsA are at risk for decreased quality of life due to both joint and skin symptoms, impaired physical function and disease progression. Treatments include non-steroidal anti-inflammatory drugs, conventional systemic disease-modifying anti-rheumatic drugs (DMARDs) such as methotrexate, and biologic agents, including tumor necrosis factor-α inhibitors. The most recently introduced treatment option is apremilast, an oral phosphodiesterase 4 inhibitor.
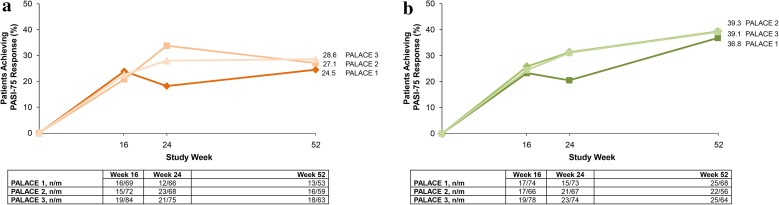
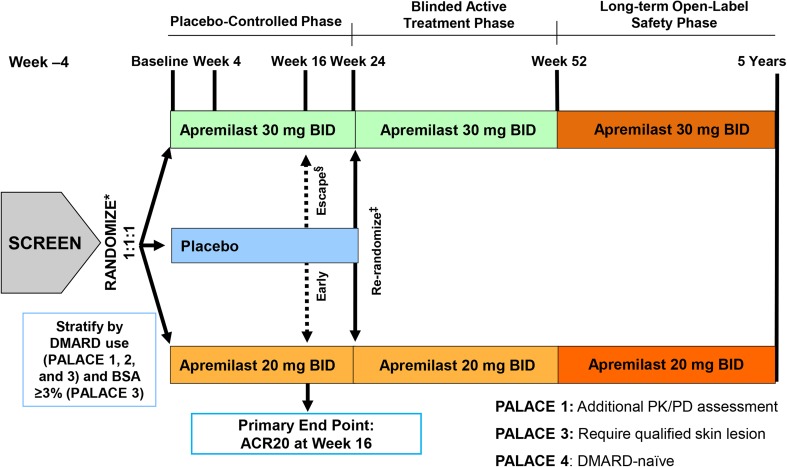
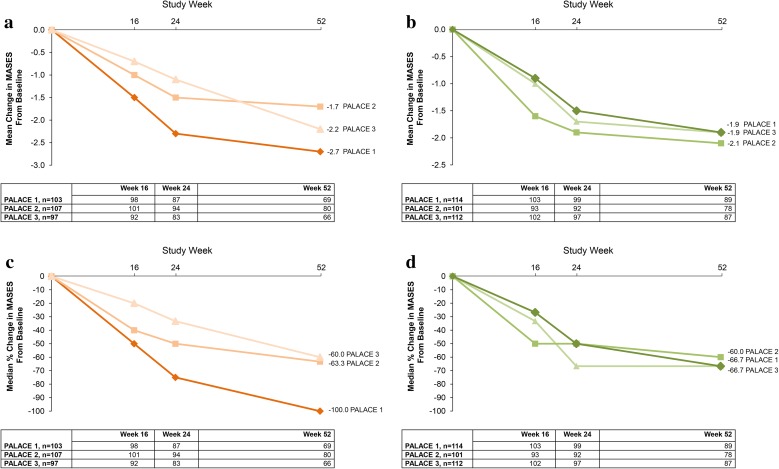
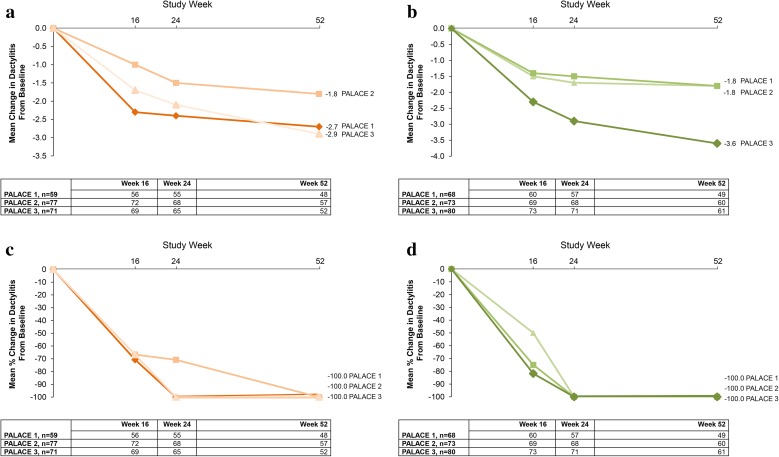
This review provides an in-depth discussion of apremilast's mechanism of action, and evidence of its clinical efficacy and safety from the Psoriatic Arthritis Long-term Assessment of Clinical Efficacy (PALACE) phase III pivotal clinical trials (PALACE 1, 2, and 3).
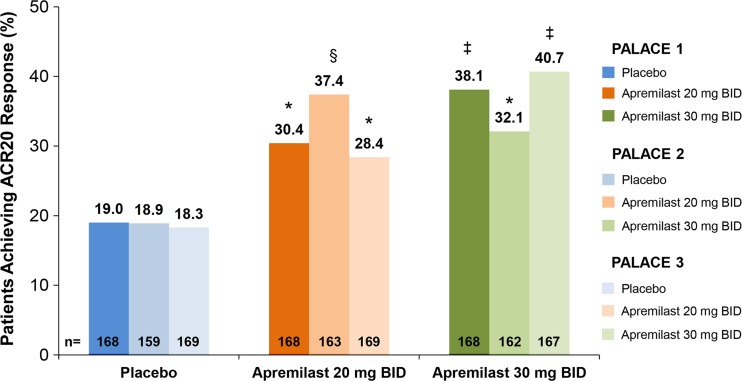
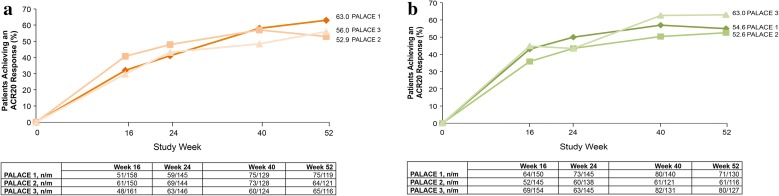
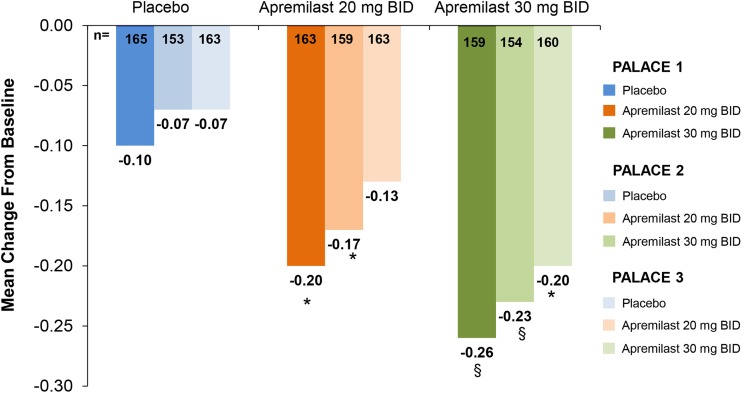
These trials demonstrate that apremilast is effective for the treatment of active PsA, despite prior conventional DMARDs or biologic treatment. The primary efficacy end point, a 20% improvement from baseline in modified American College of Rheumatology response criteria at Week 16, was achieved by significantly greater proportions of patients treated with apremilast 20 mg twice daily (BID) and apremilast 30 mg BID versus placebo in PALACE 1, 2, and 3. Improvements in this and other clinical and patient-reported end points, including swollen and tender joint counts, Psoriasis Area and Severity Index score, physical function, and quality of life, were maintained, extending over 52 weeks of treatment among patients initially randomized to apremilast. Apremilast's safety profile has been acceptable, with diarrhea and nausea being the most common adverse events, with no evidence for an increased risk of infection or need for laboratory monitoring. The PALACE pivotal data indicate that apremilast presents a new option for the treatment of PsA that may be appropriate for use early in the treatment ladder. Ongoing PALACE open-label extension trials of up to 4 years will characterize the long-term clinical effects and safety of apremilast therapy.
Celgene Corporation, Summit, NJ, USA.
银屑病关节炎(PsA)是一种脊柱关节炎,高达30%的银屑病患者会发生。由于关节和皮肤症状、身体功能受损以及疾病进展,PsA患者存在生活质量下降的风险。治疗方法包括非甾体抗炎药、传统的全身性改善病情抗风湿药(DMARDs),如甲氨蝶呤,以及生物制剂,包括肿瘤坏死因子-α抑制剂。最近推出的治疗选择是阿普斯特,一种口服磷酸二酯酶4抑制剂。
本综述深入讨论了阿普斯特的作用机制,以及来自银屑病关节炎临床疗效长期评估(PALACE)III期关键临床试验(PALACE 1、2和3)的临床疗效和安全性证据。
这些试验表明,尽管先前使用过传统DMARDs或生物治疗,阿普斯特对活动性PsA仍有效。在PALACE 1、2和3中,与安慰剂相比,每日两次服用20mg阿普斯特和每日两次服用30mg阿普斯特的患者中,达到主要疗效终点(第16周时美国风湿病学会改良反应标准较基线改善20%)的比例显著更高。这一终点以及其他临床和患者报告的终点,包括肿胀和压痛关节计数、银屑病面积和严重程度指数评分、身体功能和生活质量的改善得以维持,在最初随机分配接受阿普斯特治疗的患者中持续了52周的治疗。阿普斯特的安全性可接受,腹泻和恶心是最常见的不良事件,没有证据表明感染风险增加或需要实验室监测。PALACE关键数据表明,阿普斯特为PsA的治疗提供了一种新选择,可能适用于治疗阶梯早期使用。正在进行的长达4年的PALACE开放标签扩展试验将确定阿普斯特治疗的长期临床效果和安全性。
美国新泽西州萨默塞特的新基公司。