Pham Minh D, Agius Paul A, Romero Lorena, McGlynn Peter, Anderson David, Crowe Suzanne M, Luchters Stanley
Burnet Institute, 85 Commercial Road, Melbourne, VIC, 3004, Australia.
Department of Epidemiology and Preventive Medicine, Faculty of Medicine Nursing and Health Science, Monash University, Melbourne, Australia.
BMC Infect Dis. 2016 Oct 21;16(1):592. doi: 10.1186/s12879-016-1931-2.
Point-of-care (POC) CD4 testing increases patient accessibility to assessment of antiretroviral therapy eligibility. This review evaluates field performance in low and middle-income countries (LMICs) of currently available POC CD4 technologies.
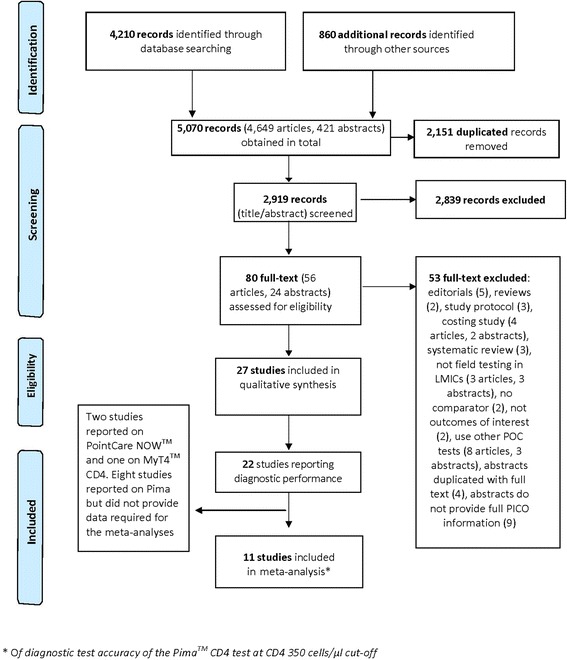
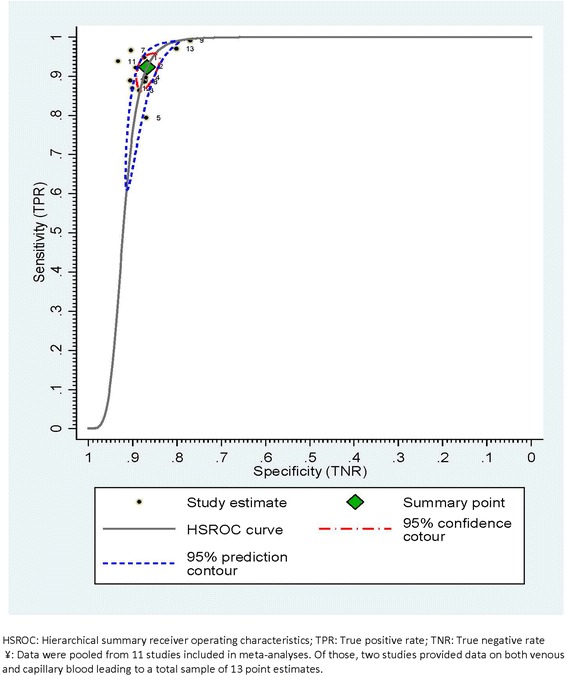
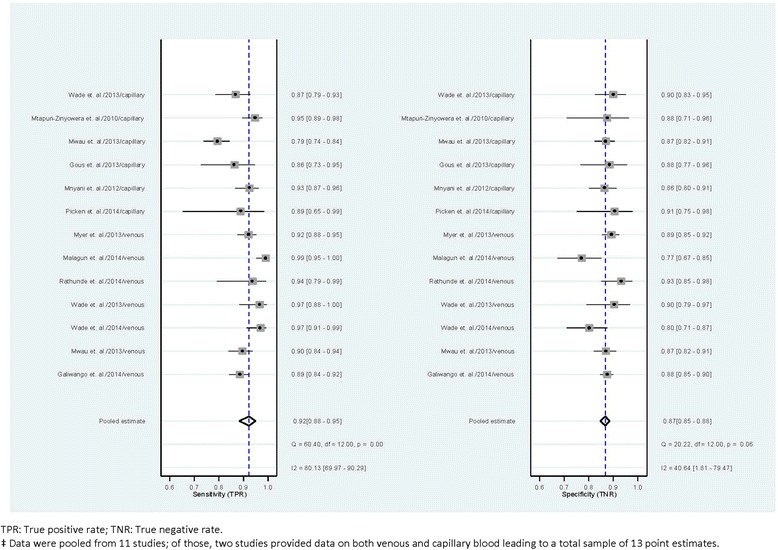
Eight electronic databases were searched for field studies published between January 2005 and January 2015 of six POC CD4 platforms: PointCare NOW™, Alere Pima™ CD4, Daktari™ CD4 Counter, CyFlow® CD4 miniPOC, BD FACSPresto™, and MyT4™ CD4. Due to limited data availability, meta-analysis was conducted only for diagnostic performance of Pima at a threshold of 350 cells/μl, applying a bivariate multi-level random-effects modelling approach. A covariate extended model was also explored to test for difference in diagnostic performance between capillary and venous blood.
Twenty seven studies were included. Published field study results were found for three of the six POC CD4 tests, 24 of which used Pima. For Pima, test failure rates varied from 2 to 23 % across study settings. Pooled sensitivity and specificity were 0.92 (95 % CI = 0.88-0.95) and 0.87 (95 % CI = 0.85-0.88) respectively. Diagnostic performance by blood sample type (venous vs. capillary) revealed non-significant differences in sensitivity (0.94 vs 0.89) and specificity (0.86 vs 0.87), respectively in the extended model (Wald χ(2) = 4.77, p = 0.09).
POC CD4 testing can provides reliable results for making treatment decision under field conditions in low-resource settings. The Pima test shows a good diagnostic performance at CD4 cut-off of 350 cells/μl. More data are required to evaluate performance of POC CD4 testing using venous versus capillary blood in LMICs which might otherwise influence clinical practice.
即时检验(POC)CD4检测增加了患者接受抗逆转录病毒治疗资格评估的可及性。本综述评估了低收入和中等收入国家(LMICs)中现有POC CD4技术的现场性能。
检索了八个电子数据库,以查找2005年1月至2015年1月期间发表的关于六个POC CD4平台的现场研究:PointCare NOW™、Alere Pima™ CD4、Daktari™ CD4计数器、CyFlow® CD4 miniPOC、BD FACSPresto™和MyT4™ CD4。由于数据可用性有限,仅对Pima在350个细胞/μl阈值下的诊断性能进行了荟萃分析,采用双变量多层次随机效应建模方法。还探索了一个协变量扩展模型,以测试毛细血管血和静脉血之间诊断性能的差异。
纳入了27项研究。在六项POC CD4检测中,有三项有已发表的现场研究结果,其中24项使用了Pima。对于Pima,在不同研究环境中,检测失败率从2%到23%不等。合并敏感性和特异性分别为0.92(95%CI = 0.88 - 0.95)和0.87(95%CI = 0.85 - 0.88)。扩展模型中,按血样类型(静脉血与毛细血管血)的诊断性能显示,敏感性(0.94对0.89)和特异性(0.86对0.87)分别无显著差异(Wald χ(2)=4.77,p = 0.09)。
POC CD4检测可为低资源环境下现场条件下的治疗决策提供可靠结果。Pima检测在CD4临界值为350个细胞/μl时显示出良好的诊断性能。需要更多数据来评估在LMICs中使用静脉血与毛细血管血进行POC CD4检测的性能,否则可能会影响临床实践。