Peeling Rosanna W, Sollis Kimberly A, Glover Sarah, Crowe Suzanne M, Landay Alan L, Cheng Ben, Barnett David, Denny Thomas N, Spira Thomas J, Stevens Wendy S, Crowley Siobhan, Essajee Shaffiq, Vitoria Marco, Ford Nathan
London School of Hygiene and Tropical Medicine, London, WC1E 7HT, England.
Centre for Biomedical Research, Burnet Institute, Melbourne, 3004, Victoria, Australia.
PLoS One. 2015 Mar 19;10(3):e0115019. doi: 10.1371/journal.pone.0115019. eCollection 2015.
Measurement of CD4+ T-lymphocytes (CD4) is a crucial parameter in the management of HIV patients, particularly in determining eligibility to initiate antiretroviral treatment (ART). A number of technologies exist for CD4 enumeration, with considerable variation in cost, complexity, and operational requirements. We conducted a systematic review of the performance of technologies for CD4 enumeration.
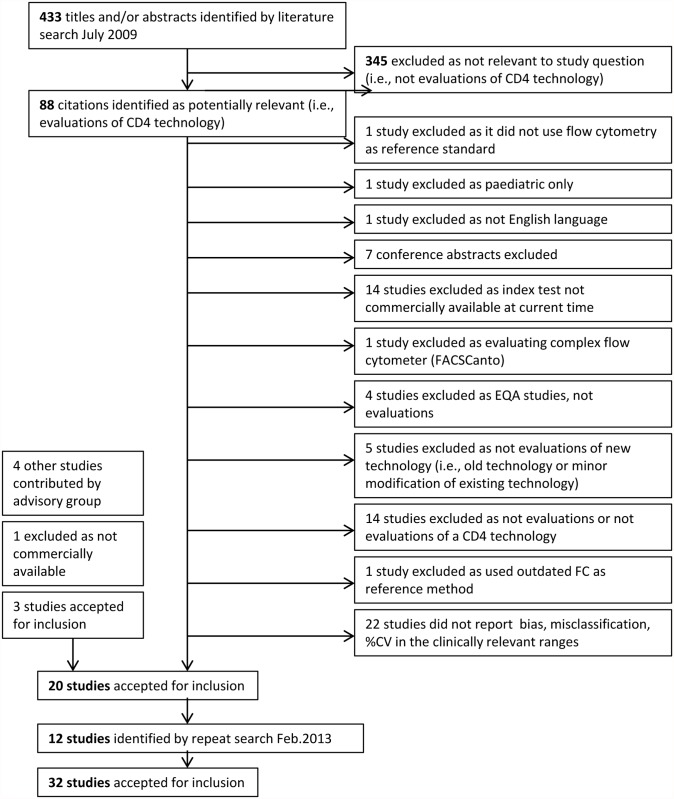
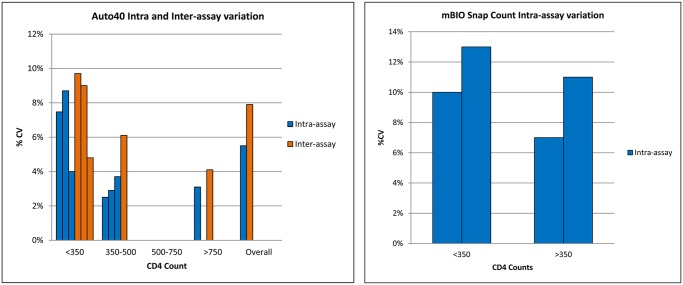
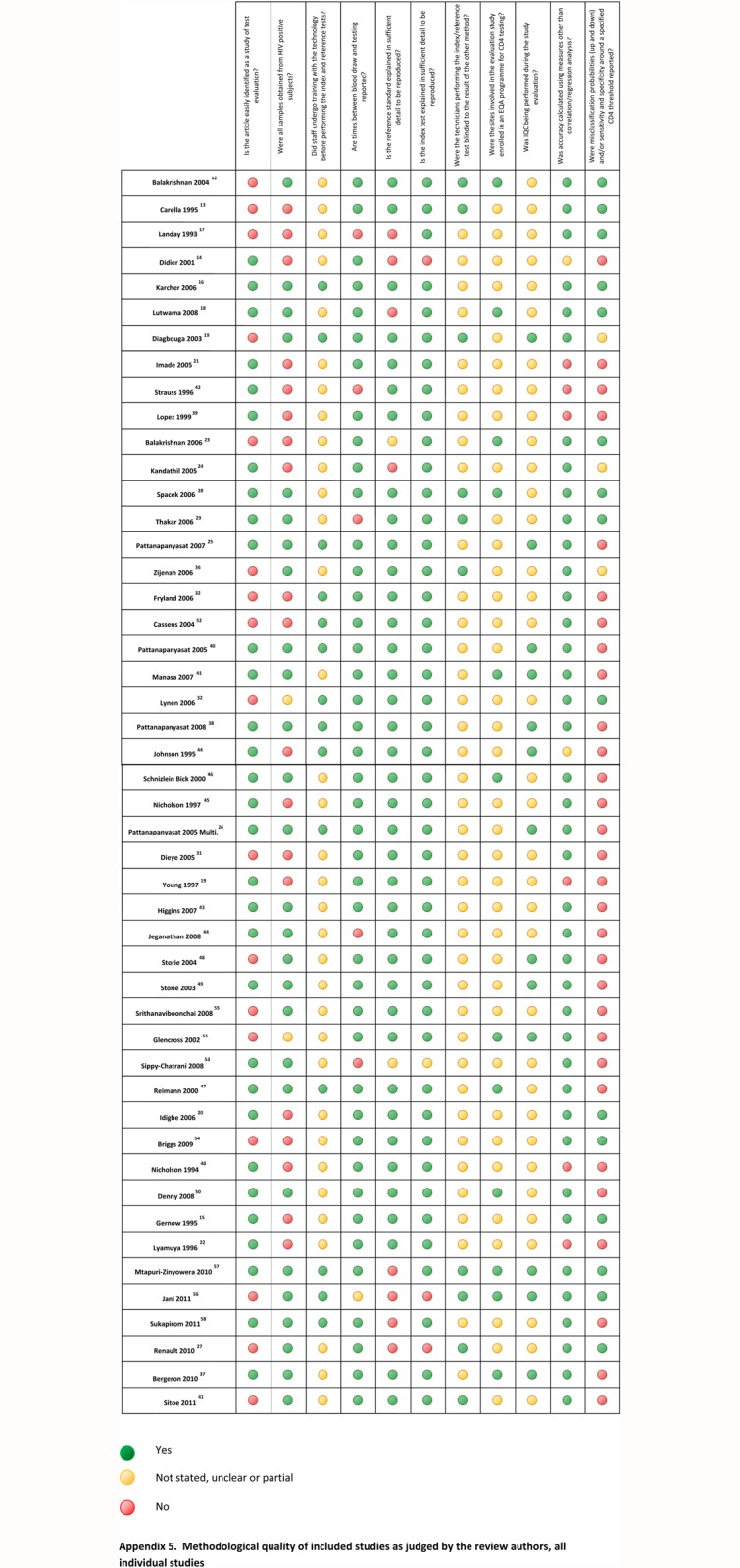
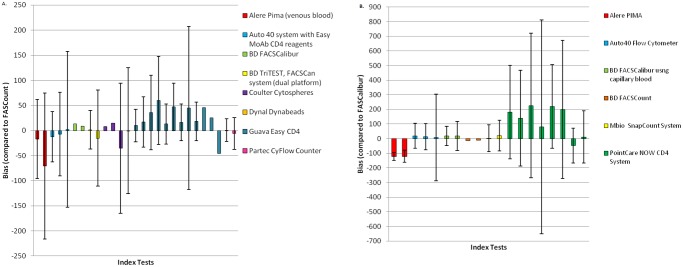
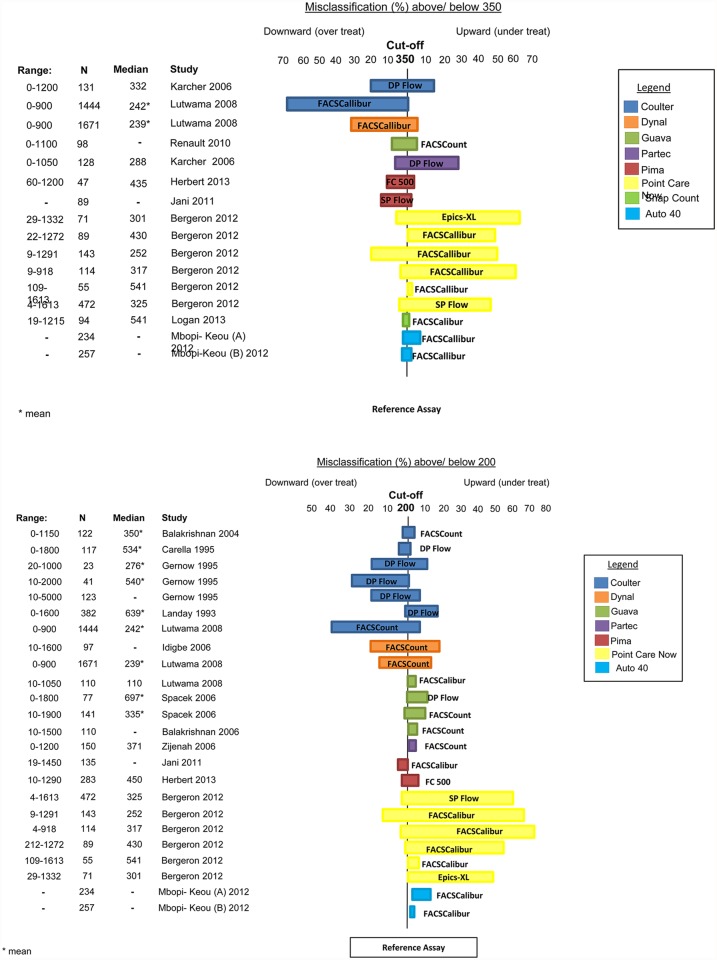
Studies were identified by searching electronic databases MEDLINE and EMBASE using a pre-defined search strategy. Data on test accuracy and precision included bias and limits of agreement with a reference standard, and misclassification probabilities around CD4 thresholds of 200 and 350 cells/μl over a clinically relevant range. The secondary outcome measure was test imprecision, expressed as % coefficient of variation. Thirty-two studies evaluating 15 CD4 technologies were included, of which less than half presented data on bias and misclassification compared to the same reference technology. At CD4 counts <350 cells/μl, bias ranged from -35.2 to +13.1 cells/μl while at counts >350 cells/μl, bias ranged from -70.7 to +47 cells/μl, compared to the BD FACSCount as a reference technology. Misclassification around the threshold of 350 cells/μl ranged from 1-29% for upward classification, resulting in under-treatment, and 7-68% for downward classification resulting in overtreatment. Less than half of these studies reported within laboratory precision or reproducibility of the CD4 values obtained.
A wide range of bias and percent misclassification around treatment thresholds were reported on the CD4 enumeration technologies included in this review, with few studies reporting assay precision. The lack of standardised methodology on test evaluation, including the use of different reference standards, is a barrier to assessing relative assay performance and could hinder the introduction of new point-of-care assays in countries where they are most needed.
CD4 + T淋巴细胞(CD4)的检测是管理HIV患者的关键参数,尤其是在确定启动抗逆转录病毒治疗(ART)的资格方面。现有多种用于CD4计数的技术,在成本、复杂性和操作要求方面存在很大差异。我们对CD4计数技术的性能进行了系统评价。
采用预定义的检索策略,通过检索电子数据库MEDLINE和EMBASE来识别研究。关于检测准确性和精密度的数据包括偏差、与参考标准的一致性界限,以及在临床相关范围内CD4阈值为200和350个细胞/μl时的错误分类概率。次要结局指标是检测不精密度,以变异系数百分比表示。纳入了32项评估15种CD4技术的研究,其中与同一参考技术相比,不到一半的研究提供了偏差和错误分类的数据。与BD FACSCount作为参考技术相比,当CD4计数<350个细胞/μl时,偏差范围为-35.2至+13.1个细胞/μl,而当计数>350个细胞/μl时,偏差范围为-70.7至+47个细胞/μl。在350个细胞/μl阈值附近,向上分类的错误分类范围为1-29%,导致治疗不足,向下分类的错误分类范围为7-68%,导致过度治疗。这些研究中不到一半报告了所获得的CD4值在实验室内部的精密度或可重复性。
本综述中纳入的CD4计数技术在治疗阈值附近报告了广泛的偏差和错误分类百分比,很少有研究报告检测精密度。检测评估缺乏标准化方法,包括使用不同的参考标准,是评估相对检测性能的障碍,并且可能阻碍在最需要的国家引入新的即时检测方法。