Prakash Sanjay, Rathore Chaturbhuj
Department of Neurology, Smt. B. K. Shah Medical institute and research Centre, Sumandeep Vidyapeeth, Piparia, Waghodia, Vadodara, 391760, Gujarat, India.
Department of Neurology, Smt B. K. Shah Medical institute and research Centre, Piperia, Waghodia, Vadodara, 391760, Gujarat, India.
J Headache Pain. 2016 Dec;17(1):95. doi: 10.1186/s10194-016-0687-9. Epub 2016 Oct 21.
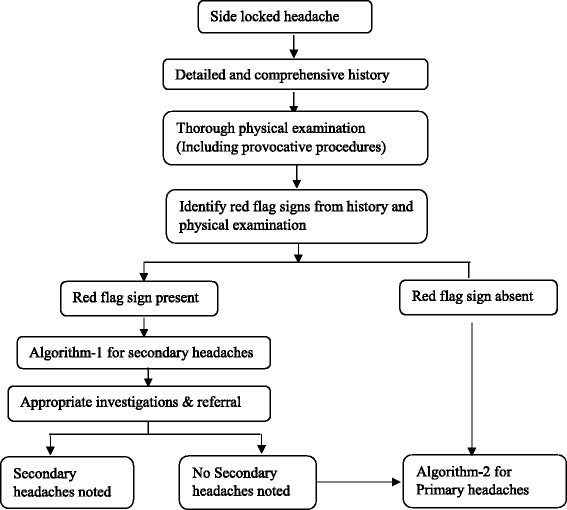
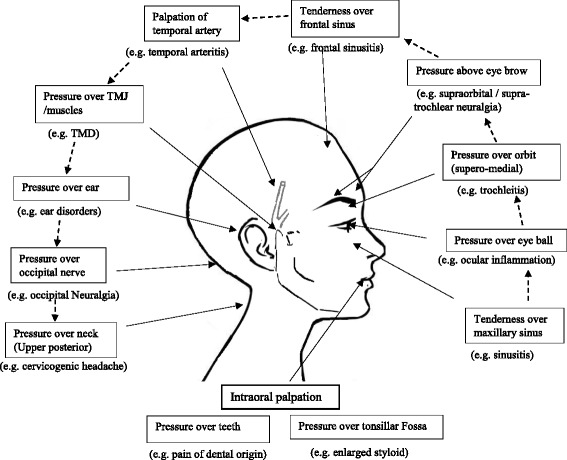
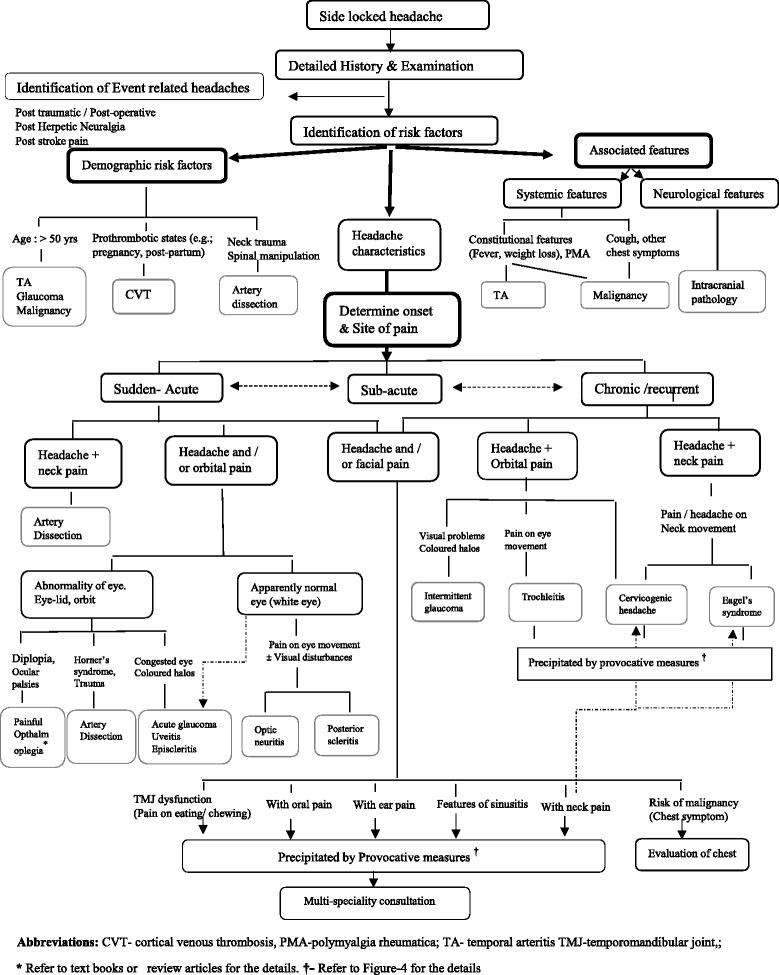
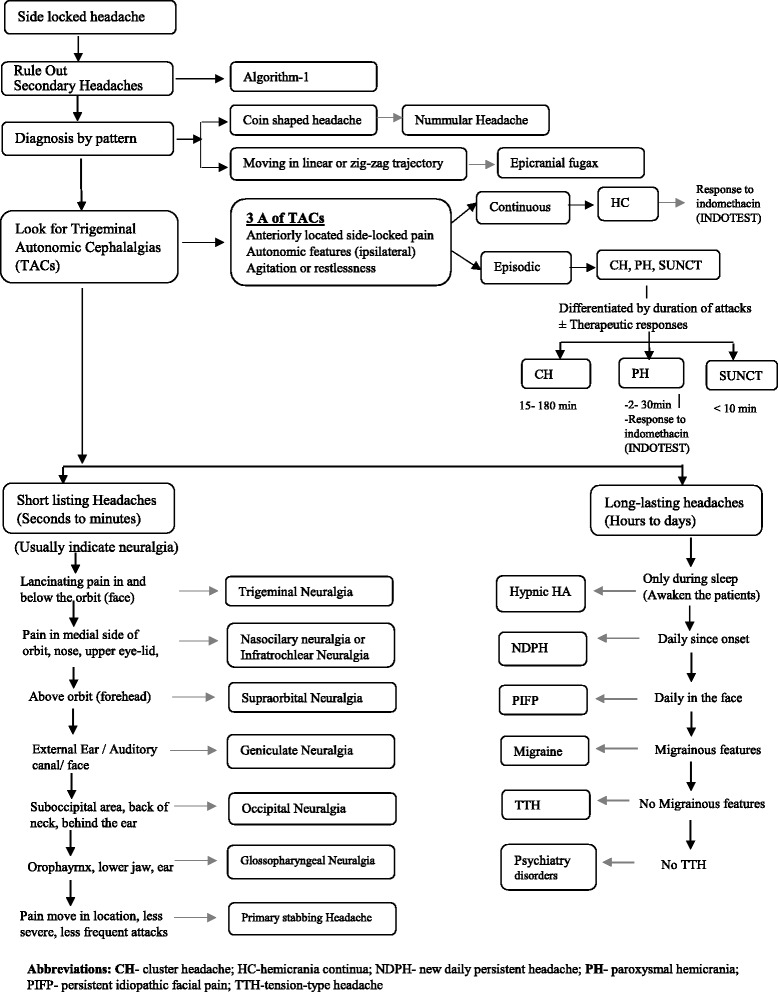
The differential diagnosis of strictly unilateral hemicranial pain includes a large number of primary and secondary headaches and cranial neuropathies. It may arise from both intracranial and extracranial structures such as cranium, neck, vessels, eyes, ears, nose, sinuses, teeth, mouth, and the other facial or cervical structure. Available data suggest that about two-third patients with side-locked headache visiting neurology or headache clinics have primary headaches. Other one-third will have either secondary headaches or neuralgias. Many of these hemicranial pain syndromes have overlapping presentations. Primary headache disorders may spread to involve the face and / or neck. Even various intracranial and extracranial pathologies may have similar overlapping presentations. Patients may present to a variety of clinicians, including headache experts, dentists, otolaryngologists, ophthalmologist, psychiatrists, and physiotherapists. Unfortunately, there is not uniform approach for such patients and diagnostic ambiguity is frequently encountered in clinical practice.Herein, we review the differential diagnoses of side-locked headaches and provide an algorithm based approach for patients presenting with side-locked headaches. Side-locked headache is itself a red flag. So, the first priority should be to rule out secondary headaches. A comprehensive history and thorough examinations will help one to formulate an algorithm to rule out or confirm secondary side-locked headaches. The diagnoses of most secondary side-locked headaches are largely investigations dependent. Therefore, each suspected secondary headache should be subjected for appropriate investigations or referral. The diagnostic approach of primary side-locked headache starts once one rule out all the possible secondary headaches. We have discussed an algorithmic approach for both secondary and primary side-locked headaches.
严格单侧半侧头痛的鉴别诊断包括大量原发性和继发性头痛以及颅神经病变。它可能源于颅内和颅外结构,如颅骨、颈部、血管、眼睛、耳朵、鼻子、鼻窦、牙齿、口腔以及其他面部或颈部结构。现有数据表明,约三分之二前往神经内科或头痛门诊就诊的一侧固定性头痛患者患有原发性头痛。另外三分之一患者则患有继发性头痛或神经痛。许多这些半侧头痛综合征的表现相互重叠。原发性头痛疾病可能蔓延至面部和/或颈部。甚至各种颅内和颅外病变可能有相似的重叠表现。患者可能会就诊于各种临床医生,包括头痛专家、牙医、耳鼻喉科医生、眼科医生、精神科医生和物理治疗师。不幸的是,对于这类患者没有统一的诊疗方法,临床实践中经常遇到诊断模糊的情况。在此,我们回顾一侧固定性头痛的鉴别诊断,并为一侧固定性头痛患者提供基于算法的诊疗方法。一侧固定性头痛本身就是一个警示信号。所以,首要任务应该是排除继发性头痛。全面的病史和详细的检查将有助于制定一个算法来排除或确诊继发性一侧固定性头痛。大多数继发性一侧固定性头痛的诊断很大程度上依赖于检查。因此,每一例疑似继发性头痛患者都应接受适当的检查或转诊。一旦排除了所有可能的继发性头痛,就开始原发性一侧固定性头痛的诊断方法。我们已经讨论了继发性和原发性一侧固定性头痛的算法诊疗方法。