Martín-Merino Elisa, Johansson Saga, Bueno Héctor, García Rodríguez Luis A
Spanish Centre for Pharmacoepidemiologic Research (CEIFE), Madrid, Spain.
AstraZeneca R&D, Mölndal, Sweden.
Pragmat Obs Res. 2012 Mar 15;3:1-9. doi: 10.2147/POR.S29557. eCollection 2012.
Discontinuation of low-dose acetylsalicylic acid (ASA) leads to an increased risk of cardiovascular and cerebrovascular events in patients taking low-dose ASA for secondary cardiovascular prevention. However, little is known about the rate of discontinuation in everyday clinical practice.
To assess the rate of low-dose ASA discontinuation in primary care, and identify factors that predict discontinuation.
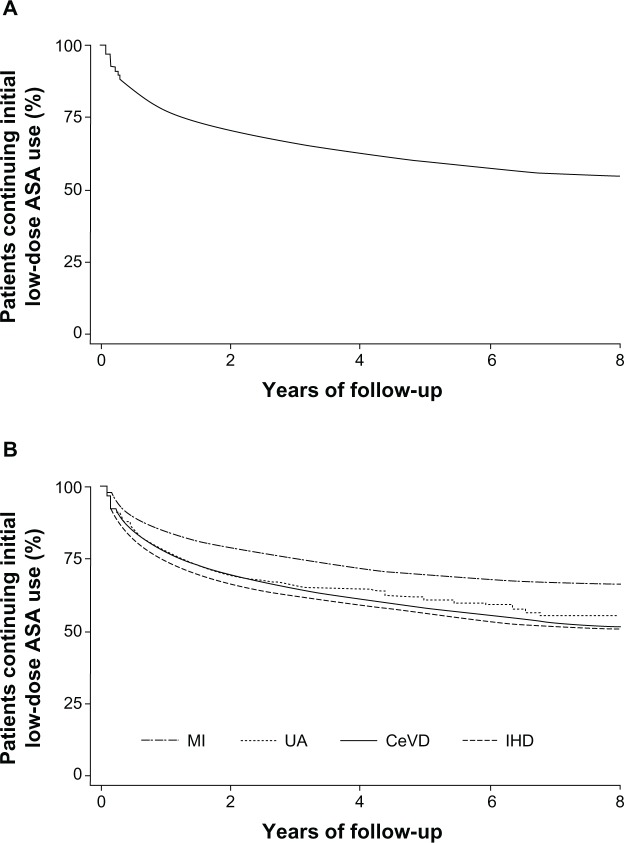
The Health Improvement Network, a large UK primary care database, was used to identify patients aged 50-84 years who received at least two consecutive prescriptions for low-dose ASA for secondary cardiovascular or cerebrovascular prevention in 2000-2007 (n = 35,639). Discontinuation was defined as a period of at least 90 days after completion of the last prescribed course of ASA during which no repeat prescription was issued.
During the study, 11,729 patients (32.9%) discontinued ASA therapy (mean follow-up 2.5 years). The discontinuation rate was lower in patients with ASA indicated for myocardial infarction than for other indications. The diagnosis of gastrointestinal disorders during the study (overall odds ratio: 1.74; 95% confidence interval: 1.61-1.88) was associated with increased rates of ASA discontinuation, whereas co-prescription of a proton pump inhibitor from the start of ASA therapy was associated with a decreased rate of discontinuation (odds ratio: 0.80; 95% confidence interval: 0.75-0.86). Co-prescription of several other cardioprotective medications was also associated with a reduced risk of discontinuation, as were increasing age, prior hospitalization and overall number of co-medications.
Continuous co-prescription of a PPI with low-dose ASA may improve adherence and outcomes, particularly in patients at both cardiovascular and gastrointestinal risk.
对于接受低剂量阿司匹林(ASA)进行二级心血管预防的患者,停用低剂量ASA会导致心血管和脑血管事件风险增加。然而,在日常临床实践中的停药率鲜为人知。
评估初级保健中低剂量ASA的停药率,并确定预测停药的因素。
利用英国一个大型初级保健数据库“健康改善网络”,识别出2000年至2007年期间年龄在50 - 84岁、接受至少两张连续低剂量ASA处方用于二级心血管或脑血管预防的患者(n = 35,639)。停药定义为在最后一次开具的ASA规定疗程结束后至少90天内未开具重复处方的时间段。
在研究期间,11,729名患者(32.9%)停用了ASA治疗(平均随访2.5年)。因心肌梗死而使用ASA的患者停药率低于其他适应症患者。研究期间诊断为胃肠道疾病(总体优势比:1.74;95%置信区间:1.61 - 1.88)与ASA停药率增加相关,而从ASA治疗开始就联合使用质子泵抑制剂与停药率降低相关(优势比:0.80;95%置信区间:0.75 - 0.86)。联合使用其他几种心脏保护药物也与停药风险降低相关,年龄增加、既往住院以及联合用药的总数也有此关联。
低剂量ASA与PPI持续联合使用可能会提高依从性和改善结局,特别是在同时存在心血管和胃肠道风险因素的患者中。