Martin Rebekah M, Cao Jie, Brisse Sylvain, Passet Virginie, Wu Weisheng, Zhao Lili, Malani Preeti N, Rao Krishna, Bachman Michael A
Department of Pathology, University of Michigan Medical School, Ann Arbor, Michigan, USA.
Institut Pasteur, Microbial Evolutionary Genomics, Paris, France.
mSphere. 2016 Oct 19;1(5). doi: 10.1128/mSphere.00261-16. eCollection 2016 Sep-Oct.
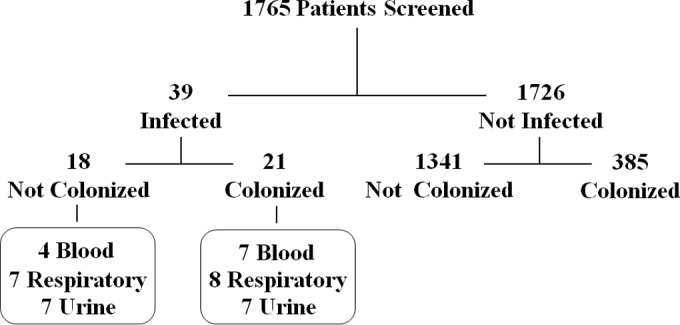
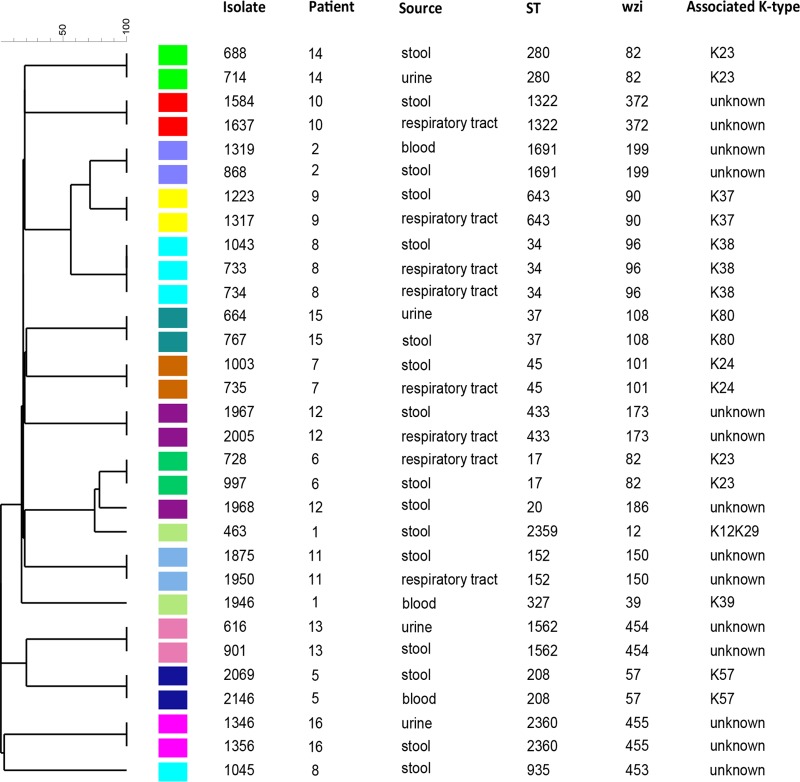
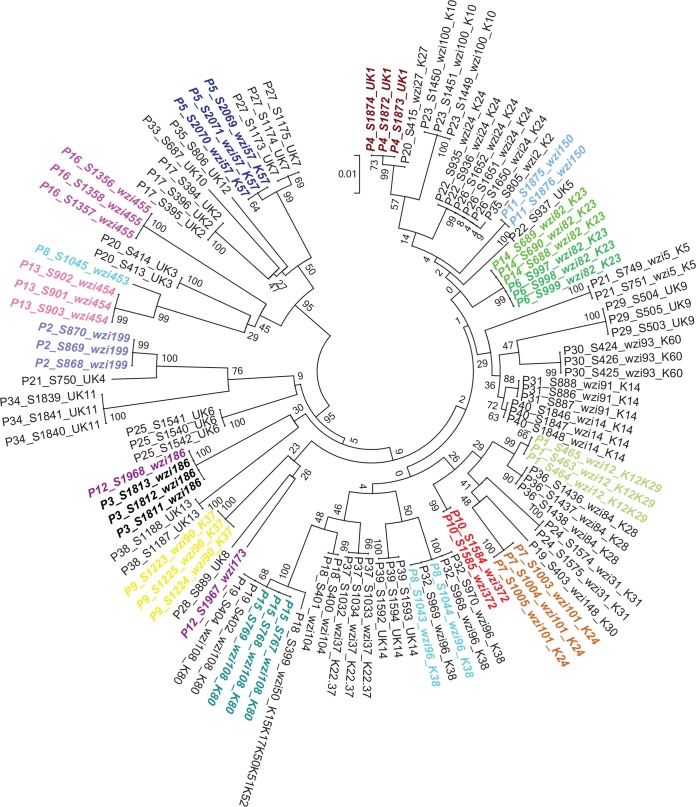
is among the most common causes of hospital-acquired infections and has emerged as an urgent threat to public health due to carbapenem antimicrobial resistance. commonly colonizes hospitalized patients and causes extraintestinal infections such as urinary tract infection, bloodstream infection (septicemia), and pneumonia. If colonization is an intermediate step before infection, then detection and characterization of colonizing isolates could enable strategies to prevent or empirically treat infections in hospitalized patients. However, the strength of the association between colonization and infection is unclear. To test the hypothesis that hospitalized patients become infected with their colonizing strain, 1,765 patients were screened for rectal colonization with , and extraintestinal isolates from these same patients were collected over a 3-month period in a cohort study design. The overall colonization prevalence was 23.0%. After adjustment for other patient factors, colonization was significantly associated with subsequent infection: 21 of 406 (5.2%) colonized patients later had extraintestinal infection, compared to 18 of 1,359 (1.3%) noncolonized patients (adjusted odds ratio [OR], 4.01; 95% confidence interval, 2.08 to 7.73; < 0.001). Despite a high diversity of colonizing isolates, 7/7 respiratory, 4/4 urinary, and 2/5 bloodstream isolates from colonized patients matched the patient corresponding rectal swab isolates, based on capsular typing, multilocus sequence typing (MLST), and whole-genome sequence analysis. These results suggest that colonization is directly associated with progression to extraintestinal infection. K. pneumoniae commonly infects hospitalized patients, and these infections are increasingly resistant to carbapenems, the antibiotics of last resort for life-threatening bacterial infections. To prevent and treat these infections, we must better understand how causes disease and discover new ways to predict and detect infections. This study demonstrates that colonization with in the intestinal tract is strongly linked to subsequent infection. This finding helps to identify a potential time frame and possible approach for intervention: the colonizing strain from a patient could be isolated as part of a risk assessment, and antibiotic susceptibility testing could guide empirical therapy if the patient becomes acutely ill.
是医院获得性感染最常见的原因之一,由于对碳青霉烯类抗菌药物耐药,已成为对公共卫生的紧迫威胁。通常定植于住院患者,并引起肠外感染,如尿路感染、血流感染(败血症)和肺炎。如果定植是感染前的中间步骤,那么对定植菌株的检测和特征分析可以使预防或经验性治疗住院患者感染的策略成为可能。然而,定植与感染之间关联的强度尚不清楚。为了检验住院患者被其定植菌株感染的假设,在一项队列研究设计中,对1765例患者进行了直肠定植筛查,并在3个月内收集了这些患者的肠外分离株。总体定植率为23.0%。在对其他患者因素进行调整后,定植与随后的感染显著相关:406例定植患者中有21例(5.2%)后来发生了肠外感染,相比之下,1359例未定植患者中有18例(1.3%)发生了肠外感染(调整后的优势比[OR]为4.01;95%置信区间为2.08至7.73;P<0.001)。尽管定植菌株具有高度多样性,但根据荚膜分型、多位点序列分型(MLST)和全基因组序列分析,来自定植患者的7/7份呼吸道、4/4份尿液和2/5份血流分离株与患者相应的直肠拭子分离株匹配。这些结果表明,肺炎克雷伯菌定植与进展为肠外感染直接相关。肺炎克雷伯菌通常感染住院患者,并且这些感染对碳青霉烯类药物的耐药性越来越高,碳青霉烯类药物是治疗危及生命的细菌感染的最后手段。为了预防和治疗这些感染,我们必须更好地了解肺炎克雷伯菌如何致病,并发现预测和检测感染的新方法。这项研究表明,肠道内肺炎克雷伯菌定植与随后的感染密切相关。这一发现有助于确定潜在的时间框架和可能的干预方法:作为风险评估的一部分,可以分离患者的定植菌株,如果患者病情急性加重,抗生素敏感性测试可以指导经验性治疗。