Lapa Constantin, Reiter Theresa, Kircher Malte, Schirbel Andreas, Werner Rudolf A, Pelzer Theo, Pizarro Carmen, Skowasch Dirk, Thomas Lena, Schlesinger-Irsch Ulrike, Thomas Daniel, Bundschuh Ralph A, Bauer Wolfgang R, Gärtner Florian C
Department of Nuclear Medicine, University Hospital Würzburg, Würzburg, Germany.
Department of Internal Medicine, University Hospital Würzburg, Würzburg, Germany.
Oncotarget. 2016 Nov 22;7(47):77807-77814. doi: 10.18632/oncotarget.12799.
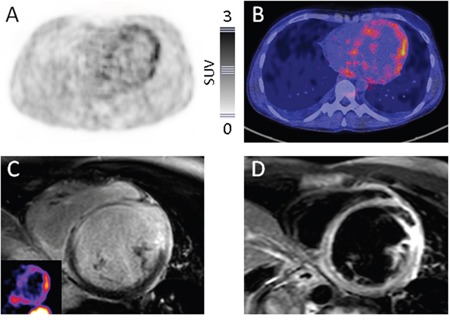
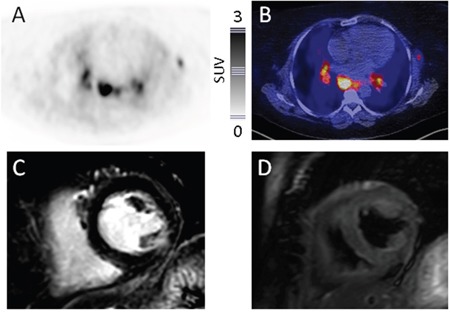
Diagnosis of cardiac sarcoidosis is often challenging. Whereas cardiac magnetic resonance imaging (CMR) and positron emission tomography/computed tomography (PET/CT) with 18F-fluorodeoxyglucose (FDG) are most commonly used to evaluate patients, PET/CT using radiolabeled somatostatin receptor (SSTR) ligands for visualization of inflammation might represent a more specific alternative. This study aimed to investigate the feasibility of SSTR-PET/CT for detecting cardiac sarcoidosis in comparison to CMR.15 patients (6 males, 9 females) with sarcoidosis and suspicion on cardiac involvement underwent SSTR-PET/CT imaging and CMR. Images were visually scored. The AHA 17-segment model of the left myocardium was used for localization and comparison of inflamed myocardium for both imaging modalities. In semi-quantitative analysis, mean (SUVmean) and maximum standardized uptake values (SUVmax) of affected myocardium were calculated and compared with both remote myocardium and left ventricular (LV) cavity.SSTR-PET was positive in 7/15, CMR in 10/15 patients. Of the 3 CMR+/PET- subjects, one patient with minor involvement (<25% of wall thickness in CMR) was missed by PET. The remaining two CMR+/PET- patients displayed no adverse cardiac events during follow-up.In the 17-segment model, PET/CT yielded 27 and CMR 29 positive segments. Overall concordance of the 2 modalities was 96.1% (245/255 segments analyzed). SUVmean and SUVmax in inflamed areas were 2.0±1.2 and 2.6±1.2, respectively. The lesion-to-remote myocardium and lesion-to-LV cavity ratios were 1.8±0.2 and 1.9±0.2 for SUVmean and 2.0±0.3 and 1.7±0.3 for SUVmax, respectively.Detection of cardiac sarcoidosis by SSTR-PET/CT is feasible. Our data warrant further analysis in larger prospective series.
心脏结节病的诊断往往具有挑战性。虽然心脏磁共振成像(CMR)和18F-氟脱氧葡萄糖(FDG)正电子发射断层扫描/计算机断层扫描(PET/CT)最常用于评估患者,但使用放射性标记的生长抑素受体(SSTR)配体进行炎症可视化的PET/CT可能是一种更具特异性的替代方法。本研究旨在探讨与CMR相比,SSTR-PET/CT检测心脏结节病的可行性。15例(6例男性,9例女性)患有结节病且怀疑有心脏受累的患者接受了SSTR-PET/CT成像和CMR检查。对图像进行视觉评分。采用美国心脏协会(AHA)左心室心肌17节段模型对两种成像方式下的炎症心肌进行定位和比较。在半定量分析中,计算受影响心肌的平均(SUVmean)和最大标准化摄取值(SUVmax),并与远隔心肌和左心室(LV)腔进行比较。SSTR-PET在7/15患者中呈阳性,CMR在10/15患者中呈阳性。在3例CMR阳性/PET阴性的患者中,PET漏诊了1例轻度受累(CMR中壁厚度<25%)的患者。其余2例CMR阳性/PET阴性患者在随访期间未出现不良心脏事件。在17节段模型中,PET/CT显示有27个阳性节段,CMR显示有29个阳性节段。两种检查方式的总体一致性为96.1%(共分析255个节段,其中245个一致)。炎症区域的SUVmean和SUVmax分别为2.0±1.2和2.6±1.2。SUVmean的病变与远隔心肌比值和病变与LV腔比值分别为1.8±0.2和1.9±0.2,SUVmax的相应比值分别为2.0±0.3和1.7±0.3。通过SSTR-PET/CT检测心脏结节病是可行的。我们的数据值得在更大规模的前瞻性研究中进一步分析。