Division of Pediatrics, UT MD Anderson Cancer Center, Houston, Texas.
Children's Oncology Group, Monrovia, California.
Pediatr Blood Cancer. 2017 Apr;64(4). doi: 10.1002/pbc.26278. Epub 2016 Oct 27.
Early response to initial chemotherapy in Hodgkin lymphoma (HL) measured by computed tomography (CT) and/or positron emission tomography (PET) after two to three cycles of chemotherapy may inform therapeutic decisions. Risk stratification at diagnosis could, however, allow earlier and potentially more efficacious treatment modifications.
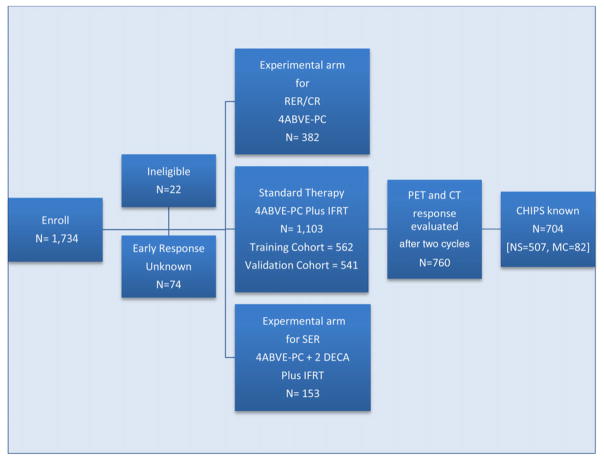
We developed a predictive model for event-free survival (EFS) in pediatric/adolescent HL using clinical data known at diagnosis from 1103 intermediate-risk HL patients treated on Children's Oncology Group protocol AHOD0031 with doxorubicin, bleomycin, vincristine, etoposide, prednisone, cyclophosphamide (ABVE-PC) chemotherapy and radiation. Independent predictors of EFS were identified and used to develop and validate a prognostic score (Childhood Hodgkin International Prognostic Score [CHIPS]). A training cohort was randomly selected to include approximately half of the overall cohort, with the remainder forming the validation cohort.
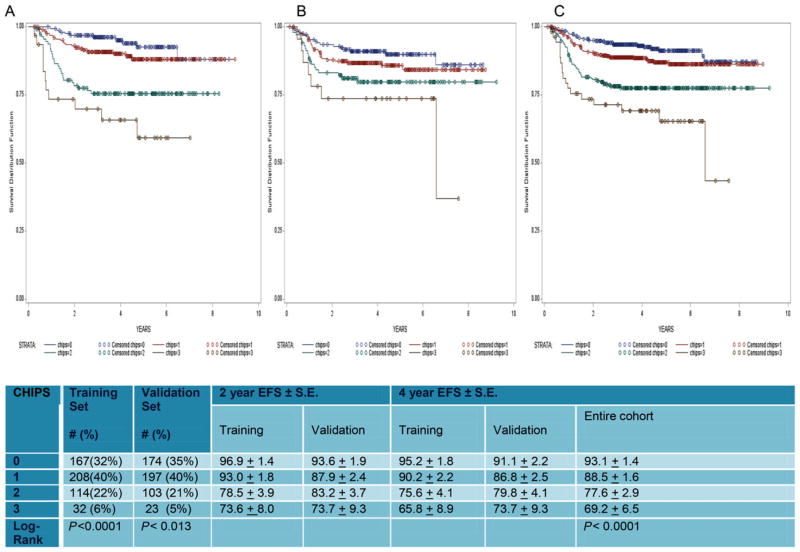
Stage 4 disease, large mediastinal mass, albumin (<3.5), and fever were independent predictors of EFS that were each assigned one point in the CHIPS. Four-year EFS was 93.1% for patients with CHIPS = 0, 88.5% for patients with CHIPS = 1, 77.6% for patients with CHIPS = 2, and 69.2% for patients with CHIPS = 3.
CHIPS was highly predictive of EFS, identifying a subset (with CHIPS 2 or 3) that comprises 27% of intermediate-risk patients who have a 4-year EFS of <80% and who may benefit from early therapeutic augmentation. Furthermore, CHIPS identified higher risk patients who were not identified by early PET or CT response. CHIPS is a robust and inexpensive approach to predicting risk in patients with intermediate-risk HL that may improve ability to tailor therapy to risk factors known at diagnosis.
霍奇金淋巴瘤(HL)患者在接受两到三个化疗周期后的计算机断层扫描(CT)和/或正电子发射断层扫描(PET)检查,可评估初始化疗的早期应答情况,从而为治疗决策提供依据。然而,在诊断时进行风险分层可以更早地进行潜在更有效的治疗调整。
我们使用 1103 例接受儿童肿瘤学组 AHOD0031 方案(阿霉素、博来霉素、长春新碱、依托泊苷、泼尼松、环磷酰胺)化疗联合放疗的中危 HL 患者的诊断时临床数据,开发了一种儿童/青少年 HL 患者无事件生存(EFS)的预测模型。确定了 EFS 的独立预测因素,并用于开发和验证预后评分(儿童霍奇金国际预后评分[CHIPS])。随机选择训练队列以纳入总队列的一半左右,其余队列则形成验证队列。
IV 期疾病、大纵隔肿块、白蛋白(<3.5)和发热是 EFS 的独立预测因素,在 CHIPS 中每个因素分别计 1 分。CHIPS=0 的患者 4 年 EFS 为 93.1%,CHIPS=1 的患者为 88.5%,CHIPS=2 的患者为 77.6%,CHIPS=3 的患者为 69.2%。
CHIPS 对 EFS 具有高度预测性,可识别出一组(CHIPS 为 2 或 3)患者,该组占中危患者的 27%,4 年 EFS<80%,可能受益于早期治疗强化。此外,CHIPS 还识别了早期 PET 或 CT 反应无法识别的高危患者。CHIPS 是一种用于预测中危 HL 患者风险的稳健且廉价的方法,可能有助于根据诊断时已知的危险因素来调整治疗方案。