Finkelstein Joseph, Friedman Carol, Hripcsak George, Cabrera Manuel
Department of Biomedical Informatics.
Department of Medicine, Columbia University College of Physicians and Surgeons, New York, NY, USA.
Pharmgenomics Pers Med. 2016 Oct 14;9:107-116. doi: 10.2147/PGPM.S117014. eCollection 2016.
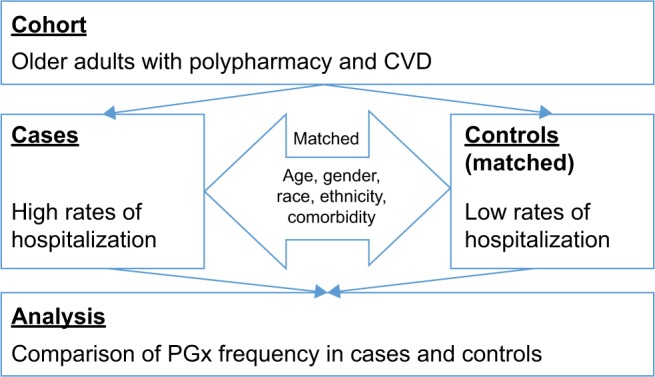
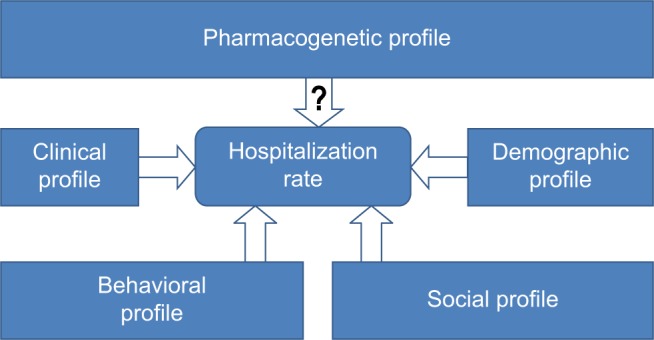
Pharmacogenetic testing identifies genetic biomarkers that are predictive of individual sensitivity to particular drugs. A significant proportion of medications that are widely prescribed for older adults are metabolized by enzymes that are encoded by highly polymorphic genes. Pharmacogenetic testing is increasingly used to optimize the medication regimen; however, its potential in older adults with polypharmacy has not been systematically explored. Following the initial case-series study, this study hypothesized that frequently hospitalized older adults with polypharmacy have higher frequency of pharmacogenetic polymorphism as compared to older adults with polypharmacy who are rarely admitted to a hospital. To test this hypothesis, a nested case-control study was conducted with pharmacogenetic polymorphism as an exposure and hospitalization rate as an outcome. In this study, frequently hospitalized older adults (≥65 years of age) with polypharmacy were matched with rarely hospitalized older adults with poly-pharmacy by age, gender, race, ethnicity, and chronic disease score. Average age and number of prescription drugs did not differ in cases and controls (77.2±5.0 and 78.3±5.1 years, 14.3±5.3 and 14.0±2.9 medications, respectively). No statistically significant difference in sociodemographic, clinical, and behavioral characteristics that are known to affect hospitalization risk was found between the cases and controls. Major pharmacogenetic polymorphism defined as presence of at least one allelic combination resulting in poor or rapid metabolizer status was identified in all the cases. No major pharmacogenetic polymorphisms were detected in controls. Based on the exact McNemar's test, the difference in major pharmacogenetic polymorphism frequency between cases and controls was statistically significant (<0.05). In 50% of cases, more than one major pharmacogenetic polymorphism was found. The frequency of CYP2C19 rapid metabolizer, CYP3A4/5 poor metabolizer, VKORC1 low sensitivity, and CYP2D6 rapid metabolizer status in cases was 67%, 33%, 33%, and 17%, respectively, which significantly exceeded respective prevalence in general population. The mean number of major gene-drug interactions found in cases was 2.8±2.2, whereas no major drug-gene interactions were identified in controls. The difference in the number of major drug-gene interactions between cases and controls was statistically significant (<0.05). The pilot data supported the hypothesis that pharmacogenetic polymorphism may represent an independent risk factor for frequent hospitalizations in older adults with polypharmacy. Due to small sample size, the results of this proof-of-concept study cannot be conclusive. Further work on the utility of pharmacogenetic testing for optimization of medication regimens in this vulnerable group of older adults is warranted.
药物遗传学检测可识别出能够预测个体对特定药物敏感性的基因生物标志物。为老年人广泛开具的药物中有很大一部分是由高度多态性基因编码的酶进行代谢的。药物遗传学检测越来越多地用于优化药物治疗方案;然而,其在患有多种药物治疗的老年人中的潜力尚未得到系统研究。继最初的病例系列研究之后,本研究假设,与很少住院的患有多种药物治疗的老年人相比,经常住院的患有多种药物治疗的老年人具有更高频率的药物遗传多态性。为验证这一假设,开展了一项巢式病例对照研究,将药物遗传多态性作为暴露因素,住院率作为结局指标。在本研究中,将经常住院的患有多种药物治疗的老年人(≥65岁)与很少住院的患有多种药物治疗的老年人按年龄、性别、种族、民族和慢性病评分进行匹配。病例组和对照组的平均年龄和处方药数量无差异(分别为77.2±5.0岁和78.3±5.1岁,14.3±5.3种和14.0±2.9种药物)。在病例组和对照组之间,未发现已知会影响住院风险的社会人口统计学、临床和行为特征存在统计学显著差异。在所有病例中均鉴定出主要药物遗传多态性,定义为存在至少一种导致代谢不良或快速代谢状态的等位基因组合。对照组未检测到主要药物遗传多态性。基于确切的McNemar检验,病例组和对照组之间主要药物遗传多态性频率的差异具有统计学显著性(<0.05)。在50%的病例中,发现了不止一种主要药物遗传多态性。病例组中CYP2C19快速代谢型、CYP3A4/5代谢不良型、VKORC1低敏感性和CYP2D6快速代谢型状态的频率分别为67%、33%、33%和17%,显著超过了一般人群中的相应患病率。病例组中发现的主要基因-药物相互作用的平均数量为2.8±2.2,而对照组未发现主要药物-基因相互作用。病例组和对照组之间主要药物-基因相互作用数量的差异具有统计学显著性(<0.05)。这些初步数据支持了这样的假设,即药物遗传多态性可能是患有多种药物治疗的老年人频繁住院的独立危险因素。由于样本量较小,这项概念验证研究的结果尚无定论。有必要进一步研究药物遗传学检测在优化这一脆弱老年人群体药物治疗方案中的效用。