Mollee Peter, Boros Samuel, Loo Dorothy, Ruelcke Jayde E, Lakis Vanessa A, Cao Kim-Anh Lê, Renaut Patricia, Hill Michelle M
Amyloidosis Centre, Princess Alexandra Hospital, Brisbane, QLD 4102 Australia.
Anatomical Pathology Department, Pathology Queensland, Princess Alexandra Hospital, Brisbane, QLD Australia.
Clin Proteomics. 2016 Oct 27;13:30. doi: 10.1186/s12014-016-9133-x. eCollection 2016.
Correct identification of the amyloidosis-causing protein is crucial for clinical management. Recently the Mayo Clinic reported laser-capture microdissection (LCM) with liquid chromatography-coupled tandem mass spectrometry (MS/MS) as a new diagnostic tool for amyloid diagnosis. Here, we report an independent implementation of this proteomic diagnostics method at the Princess Alexandra Hospital Amyloidosis Centre in Brisbane, Australia.
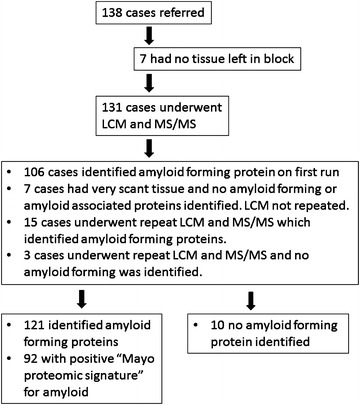
From 2010 to 2014, 138 biopsies received from 35 different organ sites were analysed by LCM-MS/MS using Congo Red staining to visualise amyloid deposits. There was insufficient tissue in the block for LCM for 7 cases. An amyloid forming protein was ultimately identified in 121 out of 131 attempted cases (94 %). Of the 121 successful cases, the Mayo Clinic amyloid proteomic signature (at least two of Serum Amyloid P, ApoE and ApoA4) was detected in 92 (76 %). Low levels of additional amyloid forming proteins were frequently identified with the main amyloid forming protein, which may reflect co-deposition of fibrils. Furthermore, vitronectin and clusterin were frequently identified in our samples. Adding vitronectin to the amyloid signature increases the number of positive cases, suggesting a potential 4th protein for the signature. In terms of clinical impact, amyloid typing by immunohistochemistry was attempted in 88 cases, reported as diagnostic in 39, however, 5 were subsequently revealed by proteomic analysis to be incorrect. Overall, the referring clinician's diagnosis of amyloid subtype was altered by proteomic analysis in 24 % of cases. While LCM-MS/MS was highly robust in protein identification, clinical information was still required for subtyping, particularly for systemic versus localized amyloidosis.
This study reports the independent implementation and evaluation of a proteomics-based diagnostic for amyloidosis subtyping. Our results support LCM-MS/MS as a powerful new diagnostic technique for amyloidosis, but also identified some challenges and further development opportunities.
正确识别导致淀粉样变性的蛋白质对于临床管理至关重要。最近,梅奥诊所报告了激光捕获显微切割(LCM)与液相色谱-串联质谱(MS/MS)联用作为淀粉样变性诊断的一种新的诊断工具。在此,我们报告了在澳大利亚布里斯班亚历山德拉公主医院淀粉样变性中心对这种蛋白质组学诊断方法的独立应用。
2010年至2014年期间,对从35个不同器官部位获取的138份活检样本进行了LCM-MS/MS分析,使用刚果红染色来观察淀粉样沉积物。有7例样本块中的组织不足以进行LCM分析。在131例尝试分析的病例中,最终有121例(94%)鉴定出了形成淀粉样蛋白的蛋白质。在这121例成功病例中,92例(76%)检测到了梅奥诊所淀粉样蛋白组学特征(血清淀粉样蛋白P、载脂蛋白E和载脂蛋白A4中至少两种)。经常发现除主要形成淀粉样蛋白的蛋白质外,还有低水平的其他形成淀粉样蛋白的蛋白质,这可能反映了纤维的共沉积。此外,在我们的样本中经常鉴定出玻连蛋白和簇集素。将玻连蛋白添加到淀粉样蛋白特征中会增加阳性病例的数量,这表明它可能是该特征的第4种潜在蛋白质。在临床影响方面,对88例病例尝试进行了免疫组织化学淀粉样蛋白分型,报告诊断为39例,然而,蛋白质组学分析随后发现其中5例诊断错误。总体而言,蛋白质组学分析改变了24%病例中转诊临床医生对淀粉样蛋白亚型的诊断。虽然LCM-MS/MS在蛋白质鉴定方面非常可靠,但亚型分类仍需要临床信息,特别是对于系统性与局限性淀粉样变性。
本研究报告了基于蛋白质组学的淀粉样变性亚型诊断方法的独立应用和评估。我们的结果支持LCM-MS/MS作为一种强大的淀粉样变性新诊断技术,但也发现了一些挑战和进一步的发展机会。