Sone Jun, Mori Keiko, Inagaki Tomonori, Katsumata Ryu, Takagi Shinnosuke, Yokoi Satoshi, Araki Kunihiko, Kato Toshiyasu, Nakamura Tomohiko, Koike Haruki, Takashima Hiroshi, Hashiguchi Akihiro, Kohno Yutaka, Kurashige Takashi, Kuriyama Masaru, Takiyama Yoshihisa, Tsuchiya Mai, Kitagawa Naoyuki, Kawamoto Michi, Yoshimura Hajime, Suto Yutaka, Nakayasu Hiroyuki, Uehara Naoko, Sugiyama Hiroshi, Takahashi Makoto, Kokubun Norito, Konno Takuya, Katsuno Masahisa, Tanaka Fumiaki, Iwasaki Yasushi, Yoshida Mari, Sobue Gen
1 Department of Neurology, Nagoya University Graduate School of Medicine, Nagoya, Aichi, Japan.
2 Department of Therapeutics for Intractable Neurological Disorders, Nagoya University Graduate School of Medicine, Nagoya, Aichi, Japan.
Brain. 2016 Dec;139(Pt 12):3170-3186. doi: 10.1093/brain/aww249. Epub 2016 Oct 25.
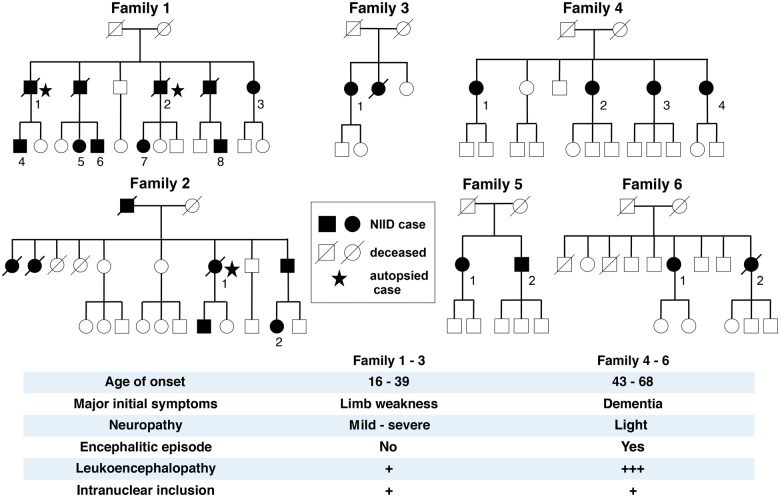
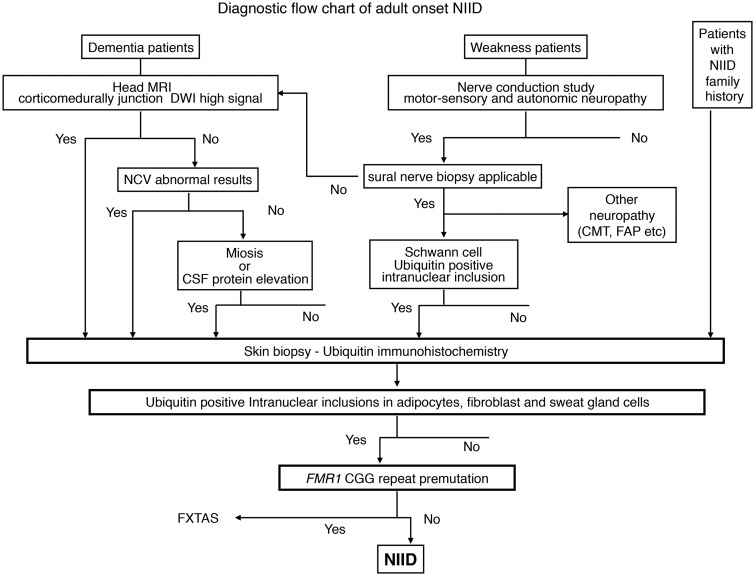
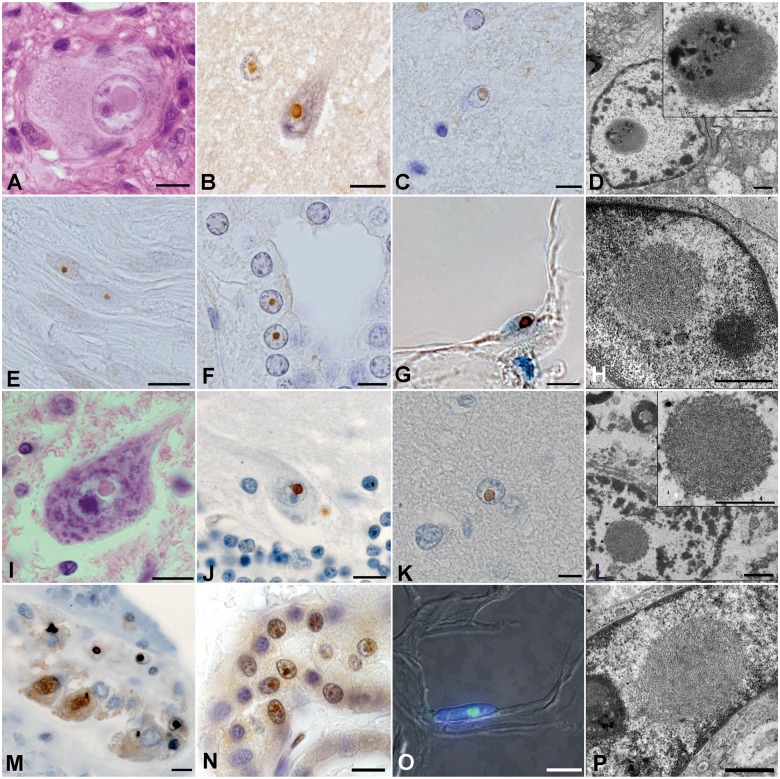
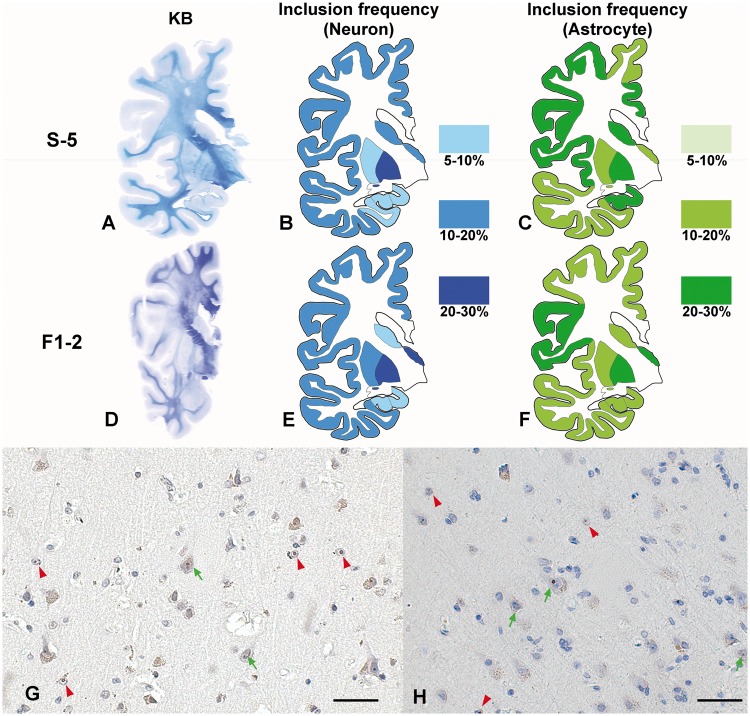
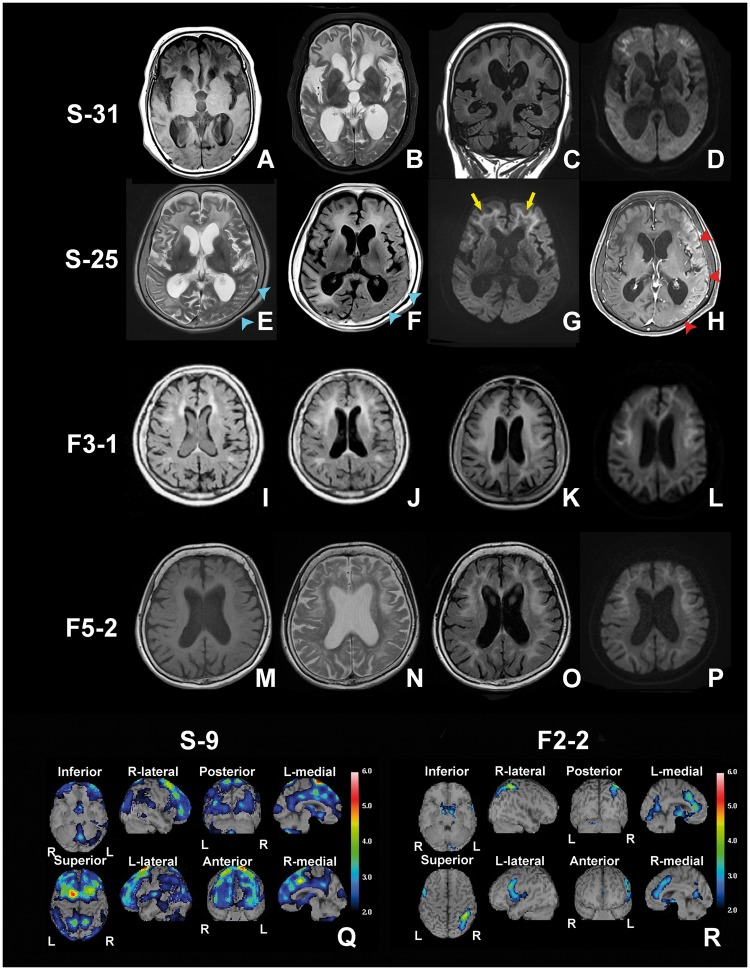
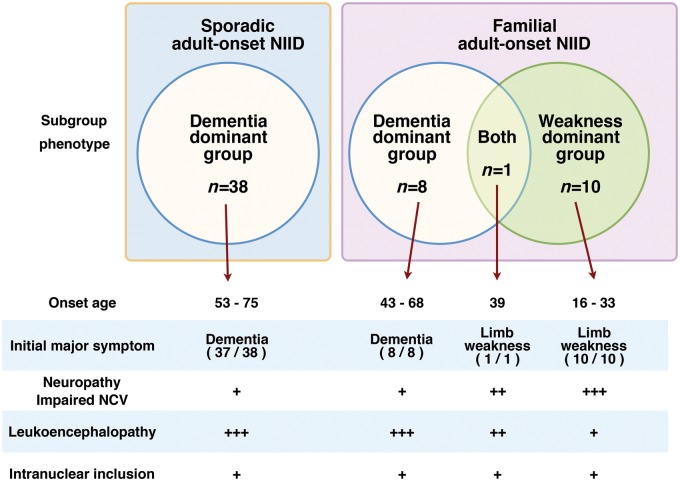
Neuronal intranuclear inclusion disease (NIID) is a slowly progressive neurodegenerative disease characterized by eosinophilic hyaline intranuclear inclusions in the central and peripheral nervous system, and also in the visceral organs. NIID has been considered to be a heterogeneous disease because of the highly variable clinical manifestations, and ante-mortem diagnosis has been difficult. However, since we reported the usefulness of skin biopsy for the diagnosis of NIID, the number of NIID diagnoses has increased, in particular adult-onset NIID. In this study, we studied 57 cases of adult-onset NIID and described their clinical and pathological features. We analysed both NIID cases diagnosed by post-mortem dissection and by ante-mortem skin biopsy based on the presence of characteristic eosinophilic, hyaline and ubiquitin-positive intanuclear inclusion: 38 sporadic cases and 19 familial cases, from six families. In the sporadic NIID cases with onset age from 51 to 76, dementia was the most prominent initial symptom (94.7%) as designated 'dementia dominant group', followed by miosis, ataxia and unconsciousness. Muscle weakness and sensory disturbance were also observed. It was observed that, in familial NIID cases with onset age less than 40 years, muscle weakness was seen most frequently (100%), as designated 'limb weakness group', followed by sensory disturbance, miosis, bladder dysfunction, and dementia. In familial cases with more than 40 years of onset age, dementia was most prominent (100%). Elevated cerebrospinal fluid protein and abnormal nerve conduction were frequently observed in both sporadic and familial NIID cases. Head magnetic resonance imaging showed high intensity signal in corticomedullary junction in diffusion-weighted image in both sporadic and familial NIID cases, a strong clue to the diagnosis. All of the dementia dominant cases presented with this type of leukoencephalopathy on head magnetic resonance imaging. Both sporadic and familial NIID cases presented with a decline in Mini-Mental State Examination and Frontal Assessment Battery scores. Based on these clinicopathological features, we proposed a diagnosis flow chart of adult-onset NIID. Our study suggested that the prevalence rate of adult-onset NIID may be higher than previously thought, and that NIID may be underdiagnosed. We should take NIID into account for differential diagnosis of leukoencephalopathy and neuropathy.
神经元核内包涵体病(NIID)是一种缓慢进展的神经退行性疾病,其特征是在中枢和周围神经系统以及内脏器官中出现嗜酸性透明核内包涵体。由于临床表现高度可变,NIID一直被认为是一种异质性疾病,生前诊断一直很困难。然而,自从我们报道皮肤活检对NIID诊断的有用性以来,NIID的诊断数量有所增加,尤其是成人发病的NIID。在本研究中,我们研究了57例成人发病的NIID病例,并描述了其临床和病理特征。我们分析了通过尸检解剖和生前皮肤活检诊断的NIID病例,这些病例均存在特征性的嗜酸性、透明和泛素阳性核内包涵体:38例散发性病例和19例家族性病例,来自6个家族。在发病年龄为51至76岁的散发性NIID病例中,痴呆是最突出的初始症状(94.7%),被指定为“痴呆主导组”,其次是瞳孔缩小、共济失调和意识丧失。还观察到肌肉无力和感觉障碍。据观察,在发病年龄小于40岁的家族性NIID病例中,最常出现肌肉无力(100%),被指定为“肢体无力组”,其次是感觉障碍、瞳孔缩小、膀胱功能障碍和痴呆。在发病年龄超过40岁的家族性病例中,痴呆最为突出(100%)。散发性和家族性NIID病例中均经常观察到脑脊液蛋白升高和神经传导异常。头部磁共振成像显示,散发性和家族性NIID病例在扩散加权图像的皮质髓质交界处均有高强度信号,这是诊断的重要线索。所有痴呆主导型病例在头部磁共振成像上均表现为这种类型的白质脑病。散发性和家族性NIID病例的简易精神状态检查表和额叶评估量表评分均下降。基于这些临床病理特征,我们提出了成人发病NIID的诊断流程图。我们的研究表明,成人发病NIID的患病率可能高于先前的认识,并且NIID可能未得到充分诊断。在对白质脑病和神经病进行鉴别诊断时,应考虑NIID。