Kamerling Cornelis Ph, Fast Martin F, Ziegenhein Peter, Menten Martin J, Nill Simeon, Oelfke Uwe
Joint Department of Physics, The Institute of Cancer Research and The Royal Marsden NHS Foundation Trust, London SM2 5NG, United Kingdom.
Med Phys. 2016 Nov;43(11):6072. doi: 10.1118/1.4965045.
This study provides a proof of concept for real-time 4D dose reconstruction for lung stereotactic body radiation therapy (SBRT) with multileaf collimator (MLC) tracking and assesses the impact of tumor tracking on the size of target margins.
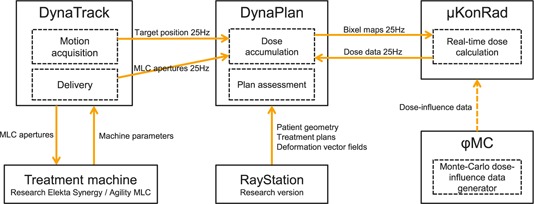
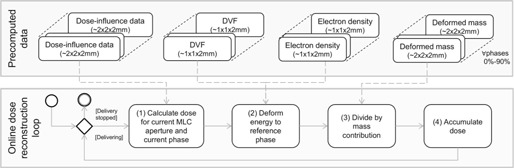
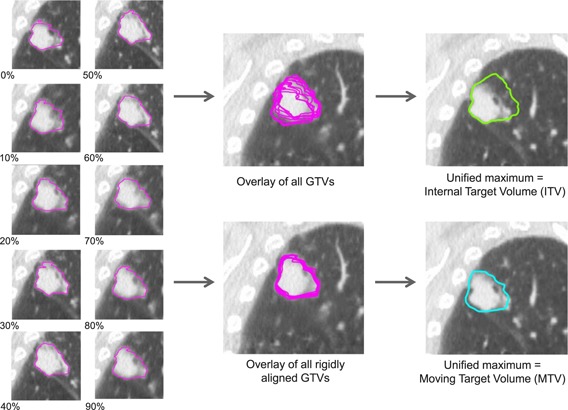
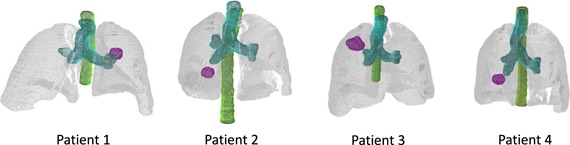
The authors have implemented real-time 4D dose reconstruction by connecting their tracking and delivery software to an Agility MLC at an Elekta Synergy linac and to their in-house treatment planning software (TPS). Actual MLC apertures and (simulated) target positions are reported to the TPS every 40 ms. The dose is calculated in real-time from 4DCT data directly after each reported aperture by utilization of precalculated dose-influence data based on a Monte Carlo algorithm. The dose is accumulated onto the peak-exhale (reference) phase using energy-mass transfer mapping. To investigate the impact of a potentially reducible safety margin, the authors have created and delivered treatment plans designed for a conventional internal target volume (ITV) + 5 mm, a midventilation approach, and three tracking scenarios for four lung SBRT patients. For the tracking plans, a moving target volume (MTV) was established by delineating the gross target volume (GTV) on every 4DCT phase. These were rigidly aligned to the reference phase, resulting in a unified maximum GTV to which a 1, 3, or 5 mm isotropic margin was added. All scenarios were planned for 9-beam step-and-shoot IMRT to meet the criteria of RTOG 1021 (3 × 18 Gy). The GTV 3D center-of-volume shift varied from 6 to 14 mm.
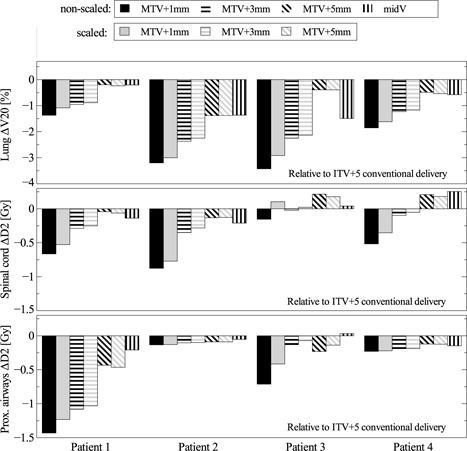
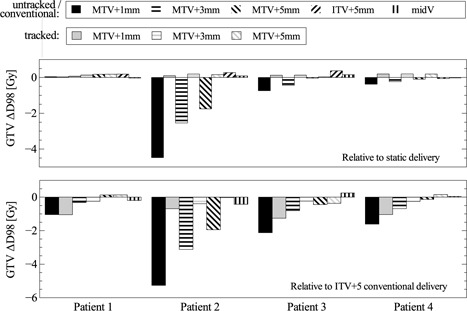
Real-time dose reconstruction at 25 Hz could be realized on a single workstation due to the highly efficient implementation of dose calculation and dose accumulation. Decreased PTV margins resulted in inadequate target coverage during untracked deliveries for patients with substantial tumor motion. MLC tracking could ensure the GTV target dose for these patients. Organ-at-risk (OAR) doses were consistently reduced by decreased PTV margins. The tracked MTV + 1 mm deliveries resulted in the following OAR dose reductions: lung V up to 3.5%, spinal cord D up to 0.9 Gy/Fx, and proximal airways D up to 1.4 Gy/Fx.
The authors could show that for patient data at clinical resolution and realistic motion conditions, the delivered dose could be reconstructed in 4D for the whole lung volume in real-time. The dose distributions show that reduced margins yield lower doses to healthy tissue, whilst target dose can be maintained using dynamic MLC tracking.
本研究为采用多叶准直器(MLC)跟踪的肺部立体定向体部放射治疗(SBRT)进行实时4D剂量重建提供了概念验证,并评估了肿瘤跟踪对靶区边缘大小的影响。
作者通过将其跟踪与输送软件连接至Elekta Synergy直线加速器的Agility MLC以及其内部治疗计划软件(TPS),实现了实时4D剂量重建。每40毫秒向TPS报告实际MLC孔径和(模拟的)靶区位置。利用基于蒙特卡罗算法预先计算的剂量影响数据,在每次报告孔径后直接根据4DCT数据实时计算剂量。使用能量-质量转移映射将剂量累积到呼气峰值(参考)相位上。为了研究潜在可缩小的安全裕度的影响,作者为4例肺部SBRT患者创建并实施了针对传统内部靶区体积(ITV)+5mm、中期通气方法以及三种跟踪方案的治疗计划。对于跟踪计划,通过在每个4DCT相位上勾勒大体靶区体积(GTV)来建立移动靶区体积(MTV)。将这些与参考相位进行刚性对齐,从而得到一个统一的最大GTV,并在其上添加1、3或5mm的各向同性边缘。所有方案均计划采用9野步进式IMRT,以满足RTOG 1021(3×18Gy)的标准。GTV的3D体积中心位移在6至14mm之间变化。
由于剂量计算和剂量累积的高效实现,可在单个工作站上以25Hz实现实时剂量重建。对于肿瘤运动较大的患者,在未跟踪输送过程中,PTV边缘减小会导致靶区覆盖不足。MLC跟踪可确保这些患者的GTV靶区剂量。PTV边缘减小可使危及器官(OAR)剂量持续降低。跟踪的MTV+1mm输送导致以下OAR剂量降低:肺V降低高达3.5%,脊髓D降低高达0.9Gy/分次,近端气道D降低高达1.4Gy/分次。
作者能够证明,对于临床分辨率和现实运动条件下的患者数据,可实时对整个肺体积进行4D剂量重建。剂量分布表明,减小边缘可降低健康组织的剂量,同时使用动态MLC跟踪可维持靶区剂量。