Chen Yu-Mu, Lai Chien-Hao, Rau Kun-Ming, Huang Cheng-Hua, Chang Huang-Chih, Chao Tung-Ying, Tseng Chia-Cheng, Fang Wen-Feng, Chung Yu-Hsiu, Wang Yi-Hsi, Su Mao-Chang, Huang Kuo-Tung, Liu Shih-Feng, Chen Hung-Chen, Chang Ya-Chun, Chang Yu-Ping, Wang Chin-Chou, Lin Meng-Chih
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Chang Gung Memorial Hospital-Kaohsiung Medical Center, Chang Gung University College of Medicine, No. 123, Ta-Pei Road, Niao-Sung District, Kaohsiung City, Taiwan.
Division of Hematology-Oncology, Department of Internal Medicine, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan.
BMC Cancer. 2016 Nov 8;16(1):868. doi: 10.1186/s12885-016-2917-6.
Epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitor (TKI) readministration to lung cancer patients is common owing to the few options available. Impact of clinical factors on prognosis of EGFR-mutant non-small cell lung cancer (NSCLC) patients receiving EGFR-TKI readministration after first-line EGFR-TKI failure and a period of TKI holiday remains unclear. Through this retrospective study, we aimed to understand the impact of clinical factors in such patients.
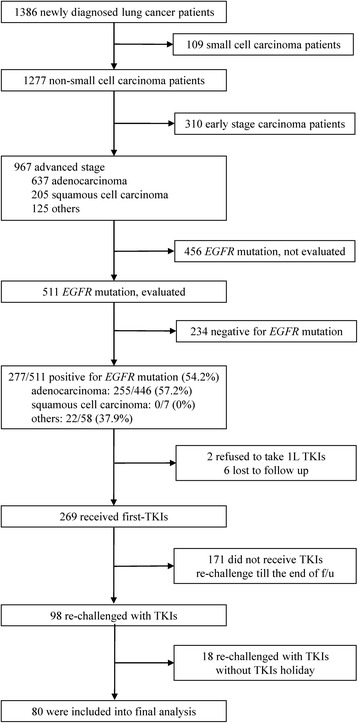
Of 1386 cases diagnosed between December 2010 and December 2013, 80 EGFR-mutant NSCLC patients who were readministered TKIs after failure of first-line TKIs and intercalated with at least one cycle of cytotoxic agent were included. We evaluated clinical factors that may influence prognosis of TKI readministration as well as systemic inflammatory status in terms of neutrophil-to-lymphocyte ratio (NLR) and lymphocyte-to-monocyte ratio (LMR). Baseline NLR and LMR were estimated at the beginning of TKI readministration and trends of NLR and LMR were change amount from patients receiving first-Line TKIs to TKIs readministration.
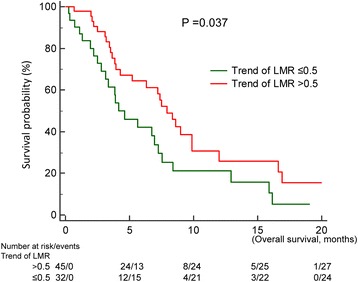
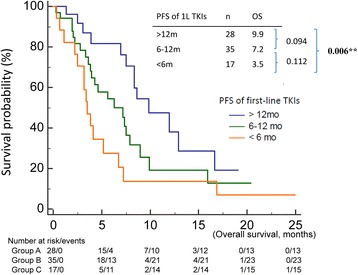
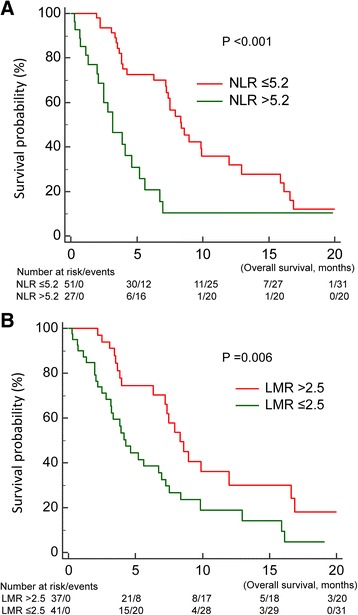
Median survival time since TKI readministration was 7.0 months. In the univariable analysis, progression free survival (PFS) of first-line TKIs, baseline NLR and LMR, and trend of LMR were prognostic factors in patients receiving TKIs readministration. In the multivariate analysis, only PFS of first-line TKIs (p < 0.001), baseline NLR (p = 0.037), and trend of LMR (p = 0.004) were prognostic factors.
Longer PFS of first-line TKIs, low baseline NLR, and high trend of LMR were good prognostic factors in EGFR-mutant NSCLC patients receiving TKI readministration.
由于可选择的治疗方案有限,肺癌患者再次使用表皮生长因子受体(EGFR)-酪氨酸激酶抑制剂(TKI)的情况很常见。临床因素对一线EGFR-TKI治疗失败并经历一段时间TKI停药期后再次接受EGFR-TKI治疗的EGFR突变非小细胞肺癌(NSCLC)患者预后的影响尚不清楚。通过这项回顾性研究,我们旨在了解这些临床因素对此类患者的影响。
在2010年12月至2013年12月期间诊断的1386例病例中,纳入了80例EGFR突变的NSCLC患者,这些患者在一线TKI治疗失败后再次接受TKI治疗,并至少接受了一个周期的细胞毒性药物治疗。我们评估了可能影响TKI再次治疗预后的临床因素以及中性粒细胞与淋巴细胞比值(NLR)和淋巴细胞与单核细胞比值(LMR)方面的全身炎症状态。在TKI再次治疗开始时估计基线NLR和LMR,NLR和LMR的变化趋势是从接受一线TKI治疗的患者到再次接受TKI治疗的患者的变化量。
自再次接受TKI治疗后的中位生存时间为7.0个月。在单变量分析中,一线TKI的无进展生存期(PFS)、基线NLR和LMR以及LMR的变化趋势是接受TKI再次治疗患者的预后因素。在多变量分析中,只有一线TKI的PFS(p<0.001)、基线NLR(p=0.037)和LMR的变化趋势(p=0.004)是预后因素。
一线TKI的PFS较长、基线NLR较低以及LMR变化趋势较高是接受TKI再次治疗的EGFR突变NSCLC患者的良好预后因素。