Winkle Roger A, Moskovitz Ryan, Mead R Hardwin, Engel Gregory, Kong Melissa H, Fleming William, Patrawala Rob A
Silicon Valley Cardiology, 1950 University Avenue, Suite 160, E. Palo Alto, CA, 94303, USA.
Sequoia Hospital, Redwood City, CA, USA.
J Interv Card Electrophysiol. 2017 Mar;48(2):177-184. doi: 10.1007/s10840-016-0207-5. Epub 2016 Nov 10.
The purpose of this study was to evaluate ultra high density-activation sequence mapping (UHD-ASM) for ablating atypical atrial flutters.
For 23 patients with 31 atypical atrial flutters (AAF), we created UHD-ASM.
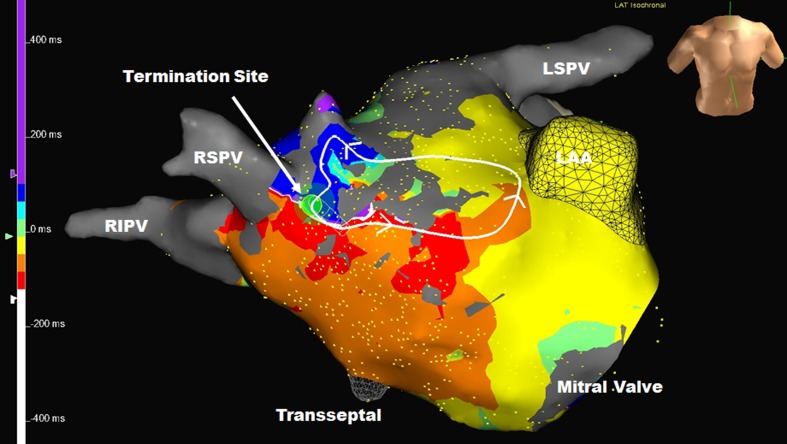
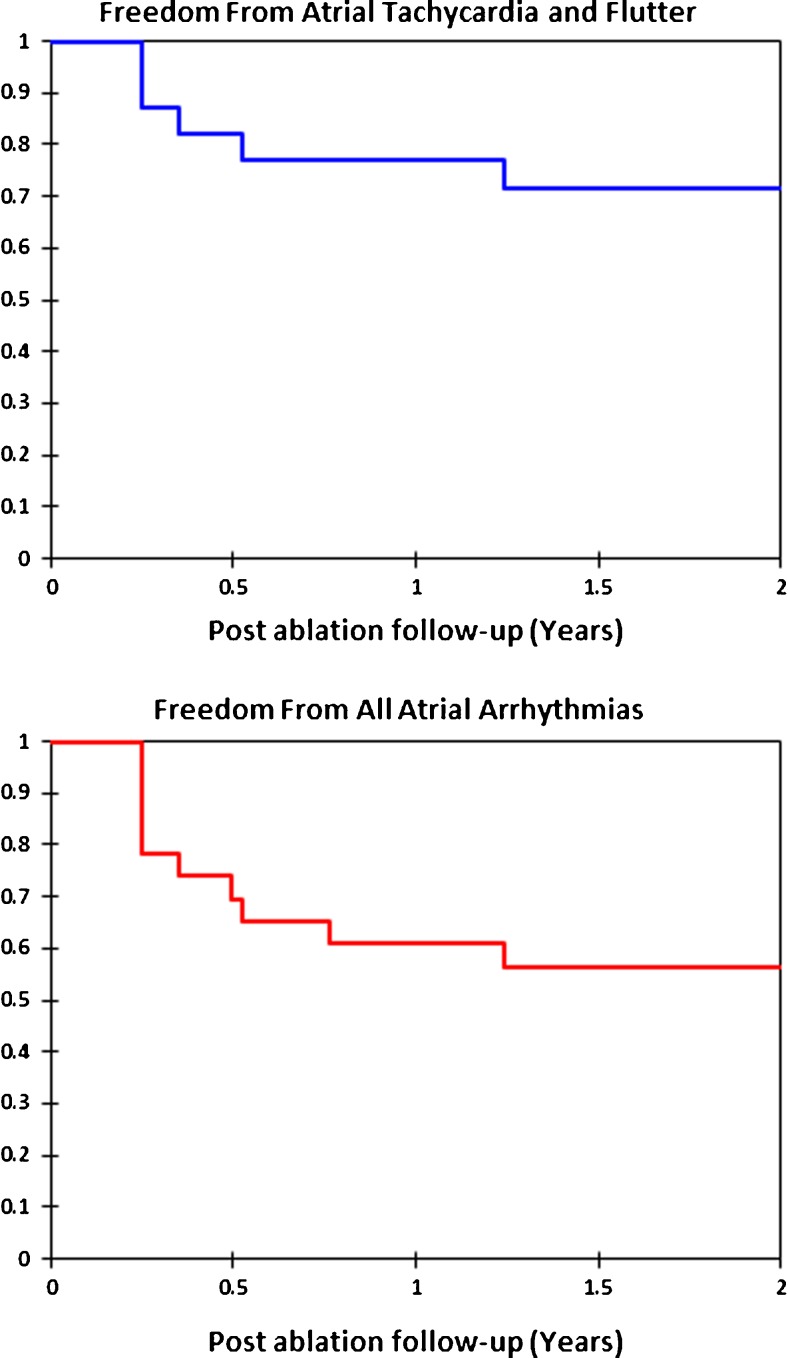
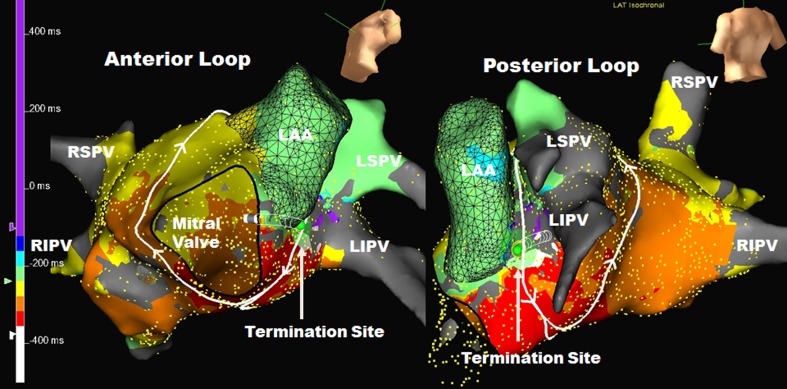
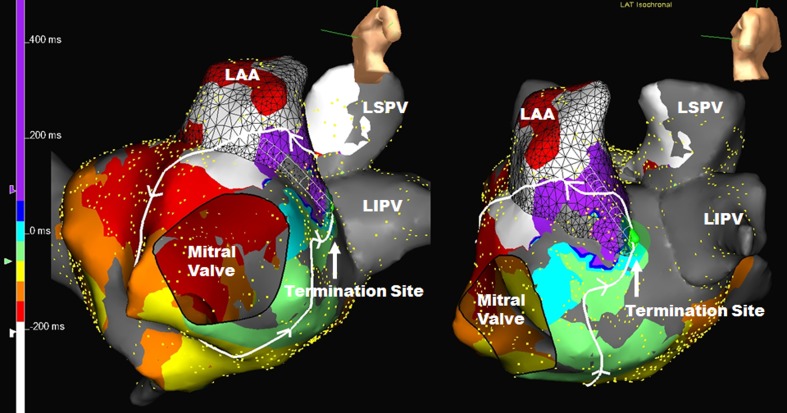
Demographics age = 65.3 ± 8.5 years, male = 78%, left atrial size = 4.66 ± 0.64 cm, redo ablation 20/23(87%). AAF were left atrial in 30 (97%). For each AAF, 1273 ± 697 points were used for UHD-ASM. Time to create and interpret the UHD-ASM was 20 ± 11 min. For every AAF, the entire circuit was identified. Thirty (97%) were macroreentry. AAF cycle length was 267 ± 49 ms, and the circuit length was 138 ± 38 mm (range 35-187). Macroreentry atrial flutters took varied pathways, but each had an area of slow conduction (ASC) averaging 16 ± 6 mm (range 6-29) in length. Entrainment was not utilized. We targeted the ASC and ablation terminated AAF directly in 19/31 (61.3%) and altered AAF activation in 7/31 (22.6%), all of which terminated directly with additional mapping/ablation. AAF degenerated to atrial fibrillation in 2/31 (6.5%) with RF and could not be reinduced after ASC ablation. Median time from initial ablation to AAF termination was 64 s. Thus, 28/31 (90.3%) terminated with RF energy and/or could not be reinduced after ASC ablation. At 1 year of follow-up, 77% were free of atrial tachycardia or atrial flutter and 61% were free of all atrial arrhythmias.
Using rapidly acquired UHD-ASM, the entire AAF circuit as well as the target ASC could be identified. Most AAF were left atrial macroreentry. Ablation of the ASC or microreentry focuses directly terminated or eliminated AAF in 90.3% without the need for entrainment mapping.
本研究旨在评估超高密度激活序列标测(UHD - ASM)用于消融非典型心房扑动的效果。
对23例患有31次非典型心房扑动(AAF)的患者,我们创建了UHD - ASM。
人口统计学数据显示,年龄 = 65.3 ± 8.5岁,男性占78%,左心房大小 = 4.66 ± 0.64 cm,再次消融的患者有20/23(87%)。30例(97%)的AAF起源于左心房。对于每例AAF,UHD - ASM使用了1273 ± 697个点。创建和解读UHD - ASM的时间为20 ± 11分钟。对于每例AAF,整个折返环均被识别。30例(97%)为大折返。AAF的周长为267 ± 49毫秒,折返环长度为138 ± 38毫米(范围35 - 187)。大折返性心房扑动走行路径各异,但每条均有一个平均长度为16 ± 6毫米(范围6 - 29)的缓慢传导区(ASC)。未使用拖带标测。我们将靶点定位于ASC,消融直接终止了19/31(61.3%)的AAF,并改变了7/31(22.6%)的AAF激活,所有这些在额外标测/消融后均直接终止。2/31(6.5%)的AAF在射频消融时恶化为心房颤动,在ASC消融后无法再次诱发。从初次消融到AAF终止的中位时间为64秒。因此,28/31(90.3%)在射频能量作用下终止和/或在ASC消融后无法再次诱发。在1年的随访中,77%的患者无房性心动过速或心房扑动,61%的患者无所有房性心律失常。
使用快速获取的UHD - ASM,可识别整个AAF折返环以及靶点ASC。大多数AAF为左心房大折返。消融ASC或微折返灶可直接终止或消除90.3%的AAF,无需拖带标测。