Alton Eric W F W, Beekman Jeffery M, Boyd A Christopher, Brand June, Carlon Marianne S, Connolly Mary M, Chan Mario, Conlon Sinead, Davidson Heather E, Davies Jane C, Davies Lee A, Dekkers Johanna F, Doherty Ann, Gea-Sorli Sabrina, Gill Deborah R, Griesenbach Uta, Hasegawa Mamoru, Higgins Tracy E, Hironaka Takashi, Hyndman Laura, McLachlan Gerry, Inoue Makoto, Hyde Stephen C, Innes J Alastair, Maher Toby M, Moran Caroline, Meng Cuixiang, Paul-Smith Michael C, Pringle Ian A, Pytel Kamila M, Rodriguez-Martinez Andrea, Schmidt Alexander C, Stevenson Barbara J, Sumner-Jones Stephanie G, Toshner Richard, Tsugumine Shu, Wasowicz Marguerite W, Zhu Jie
Department of Gene Therapy, National Heart and Lung Institute, Imperial College London, London, UK.
UK Cystic Fibrosis Gene Therapy Consortium, Oxford, UK.
Thorax. 2017 Feb;72(2):137-147. doi: 10.1136/thoraxjnl-2016-208406. Epub 2016 Nov 16.
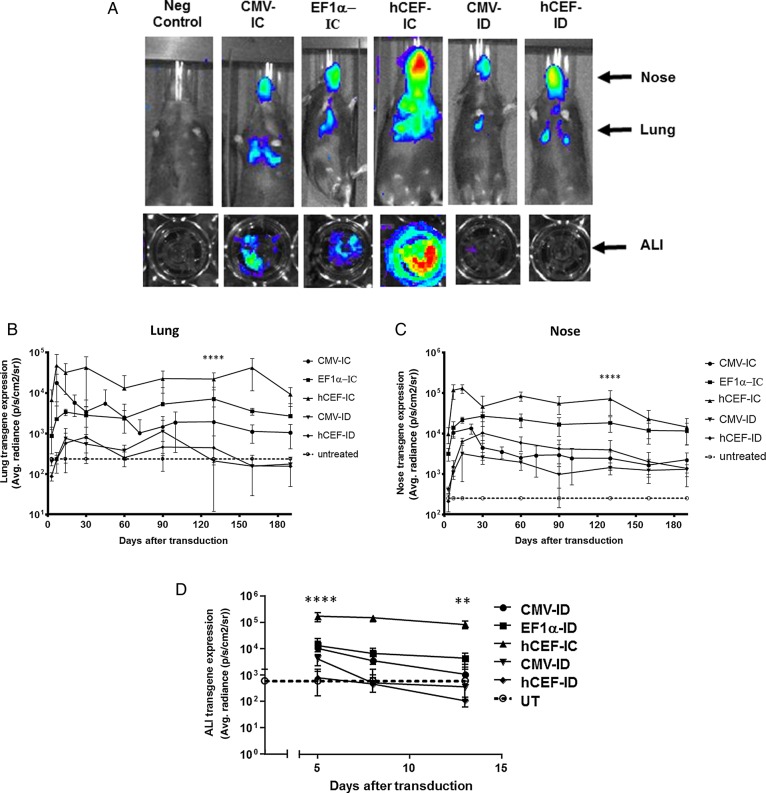
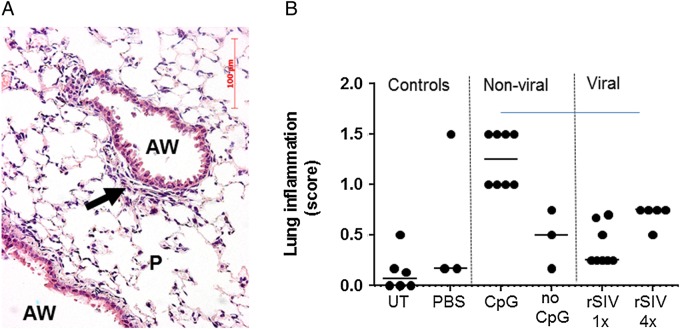
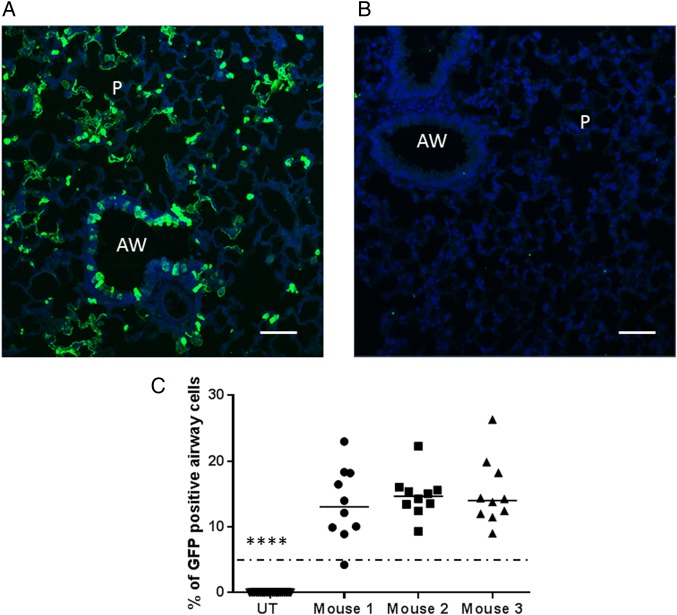
We have recently shown that non-viral gene therapy can stabilise the decline of lung function in patients with cystic fibrosis (CF). However, the effect was modest, and more potent gene transfer agents are still required. Fuson protein (F)/Hemagglutinin/Neuraminidase protein (HN)-pseudotyped lentiviral vectors are more efficient for lung gene transfer than non-viral vectors in preclinical models. In preparation for a first-in-man CF trial using the lentiviral vector, we have undertaken key translational preclinical studies. Regulatory-compliant vectors carrying a range of promoter/enhancer elements were assessed in mice and human air-liquid interface (ALI) cultures to select the lead candidate; cystic fibrosis transmembrane conductance receptor (CFTR) expression and function were assessed in CF models using this lead candidate vector. Toxicity was assessed and 'benchmarked' against the leading non-viral formulation recently used in a Phase IIb clinical trial. Integration site profiles were mapped and transduction efficiency determined to inform clinical trial dose-ranging. The impact of pre-existing and acquired immunity against the vector and vector stability in several clinically relevant delivery devices was assessed. A hybrid promoter hybrid cytosine guanine dinucleotide (CpG)- free CMV enhancer/elongation factor 1 alpha promoter (hCEF) consisting of the elongation factor 1α promoter and the cytomegalovirus enhancer was most efficacious in both murine lungs and human ALI cultures (both at least 2-log orders above background). The efficacy (at least 14% of airway cells transduced), toxicity and integration site profile supports further progression towards clinical trial and pre-existing and acquired immune responses do not interfere with vector efficacy. The lead rSIV.F/HN candidate expresses functional CFTR and the vector retains 90-100% transduction efficiency in clinically relevant delivery devices. The data support the progression of the F/HN-pseudotyped lentiviral vector into a first-in-man CF trial in 2017.
我们最近发现,非病毒基因疗法可稳定囊性纤维化(CF)患者肺功能的下降。然而,效果并不显著,仍需要更有效的基因传递载体。在临床前模型中,融合蛋白(F)/血凝素/神经氨酸酶蛋白(HN)假型慢病毒载体比非病毒载体在肺基因传递方面更有效。为准备使用慢病毒载体进行首次人体CF试验,我们开展了关键的转化临床前研究。在小鼠和人空气-液体界面(ALI)培养物中评估携带一系列启动子/增强子元件且符合监管要求的载体,以选择主要候选载体;使用该主要候选载体在CF模型中评估囊性纤维化跨膜传导调节因子(CFTR)的表达和功能。评估毒性,并与最近用于IIb期临床试验的领先非病毒制剂进行“对比”。绘制整合位点图谱并确定转导效率,为临床试验剂量范围提供依据。评估了针对载体的预先存在和获得性免疫的影响以及载体在几种临床相关递送装置中的稳定性。由伸长因子1α启动子和巨细胞病毒增强子组成的混合启动子——无混合胞嘧啶鸟嘌呤二核苷酸(CpG)的CMV增强子/伸长因子1α启动子(hCEF)在小鼠肺和人ALI培养物中均最有效(均比背景高至少2个对数级)。其疗效(至少14%的气道细胞被转导)、毒性和整合位点图谱支持进一步推进至临床试验,且预先存在和获得性免疫反应不会干扰载体疗效。主要候选载体rSIV.F/HN表达功能性CFTR,且该载体在临床相关递送装置中保留90 - 100%的转导效率。这些数据支持F/HN假型慢病毒载体在2017年进入首次人体CF试验。