Marfatia Yogesh S, Menon Devi Sathianadha, Jose Sheethal, Patel Brijesh Kumar
Department of Skin-VD, Baroda Medical College and SSG Hospital, Vadodara, Gujarat, India.
Indian J Sex Transm Dis AIDS. 2016 Jul-Dec;37(2):197-200. doi: 10.4103/0253-7184.192130.
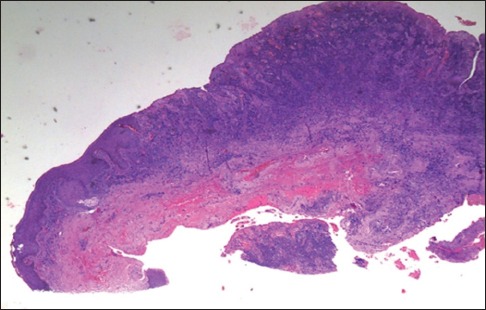
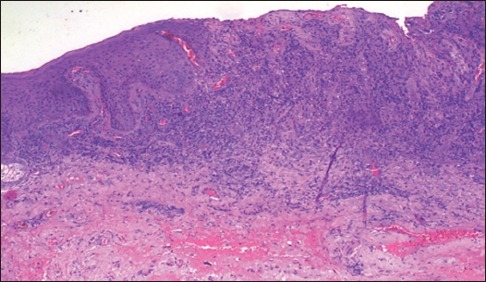
HIV/AIDS-related immune alteration poses many diagnostic and therapeutic challenges. HIV-positive 44-year-old male, on second-line antiretroviral therapy (ART) presented with asymptomatic non healing, well-defined, erythematous ulcer over penis since 8 months with serosanguinous discharge. Inguinal lymph nodes were not palpable. Tzanck smear was negative. Biopsy was not done as the patient was not willing for the same. Acyclovir was given considering herpes infection to which there was no response, and hence azithromycin and metronidazole were given, without improvement. Minocycline was given to take care of possible atypical mycobacterial infection. Due to lack of response, corticosteroid was given for 2 weeks keeping in mind possibility of vasculitis, but there was no improvement. Although investigations to rule out tuberculous etiology were negative, empirical anti-Koch's therapy Category 2 was given without response even after 3 months. Finally, a biopsy was taken from lesion which was suggestive of donovanosis. Trimethoprim Sulfamethoxazole in higher dose was started to which he responded after 2 weeks, and therapy was continued till complete response. Patient is on second-line ART for last 7 years. He is clinically stable, but his CD4 count is hovering at around 250-300 suggestive of ART failure. Virological evaluation was not feasible. Diagnostic challenges posed include possibility of resistant bacterial, viral infection, vasculitis, or drug reaction in a setting of probable ART failure.
与人类免疫缺陷病毒/获得性免疫缺陷综合征(HIV/AIDS)相关的免疫改变带来了许多诊断和治疗方面的挑战。一名44岁的HIV阳性男性,正在接受二线抗逆转录病毒疗法(ART),自8个月前起阴茎上出现无症状、不愈合、边界清晰的红斑性溃疡,并伴有血清样分泌物。腹股沟淋巴结未触及。Tzanck涂片检查结果为阴性。由于患者不愿意,未进行活检。考虑到疱疹感染给予了阿昔洛韦,但无反应,因此给予了阿奇霉素和甲硝唑,仍无改善。给予米诺环素以处理可能的非典型分枝杆菌感染。由于没有反应,考虑到血管炎的可能性给予了2周的皮质类固醇治疗,但仍无改善。尽管排除结核病因的检查结果为阴性,但给予经验性二线抗结核治疗3个月后仍无反应。最后,从病变处取活检,提示为杜诺凡病。开始使用高剂量的复方新诺明,2周后患者有反应,治疗持续至完全缓解。患者在过去7年中一直在接受二线ART治疗。他临床稳定,但其CD4细胞计数徘徊在250 - 300左右,提示ART治疗失败。病毒学评估不可行。所面临的诊断挑战包括在可能的ART治疗失败情况下存在耐药细菌、病毒感染、血管炎或药物反应的可能性。