Li Shuhua, Rong Hengmo, Guo Qinliang, Chen Yifei, Zhang Guqing, Yang Jiong
Department of Respiratory, Zhongnan Hospital of Wuhan University, Wuhan, China.
Department of Laboratory, Zhongnan Hospital of Wuhan University, Wuhan, China.
J Res Med Sci. 2016 Jun 14;21:39. doi: 10.4103/1735-1995.183996. eCollection 2016.
Serum procalcitonin (PCT) levels differ in patients with bacterial or fungal infections and are significantly elevated in patients with Gram-negative bacteremia. We evaluated the diagnostic accuracy of different inflammatory markers to discriminate sepsis caused by different pathogens.
We included 328 episodes of bacteremia from 292 patients with sepsis and 31 patients with suspected sepsis in this study. Medical records of patients who had bacteremia caused by Gram-negative bacteria (Gram-negative), Gram-positive bacteria (Gram-positive) or fungi were reviewed, and information about PCT and other inflammatory markers was recorded. The diagnostic performance of inflammatory markers was calculated via receiver operating characteristic (ROC) curves.
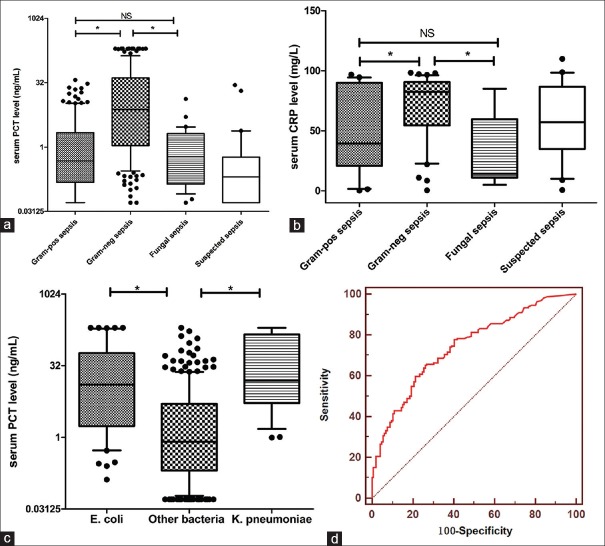
Serum PCT levels in Gram-negative, Gram-positive, and fungal sepsis were 7.47 (interquartile range [IQR]: 1.09-41.26) ng/mL, 0.48 (IQR: 0.15-2.16) ng/mL, and 0.60 (IQR: 0.14-2.06) ng/mL, respectively ( < 0.001). ROC analysis revealed an optimal cut-off value of 2.44 ng/mL for PCT in discriminating Gram-negative sepsis from Gram-positive sepsis, which yielded a sensitivity of 68.4% and a specificity of 77.1%. An optimal cut-off value of 3.11 ng/mL for PCT in discriminating Gram-negative sepsis from fungal sepsis, led to a sensitivity of 63.9% and specificity of 93.3%. Neither PCT nor other inflammatory markers could be used to distinguish between Gram-positive and fungal sepsis.
Serum PCT levels were significantly higher in patients with Gram-negative sepsis than in those with Gram-positive or fungal sepsis. PCT is a potential sensitive biomarker for distinguishing Gram-negative sepsis from Gram-positive and fungal sepsis.
细菌或真菌感染患者的血清降钙素原(PCT)水平有所不同,革兰氏阴性菌血症患者的血清PCT水平显著升高。我们评估了不同炎症标志物对鉴别由不同病原体引起的脓毒症的诊断准确性。
本研究纳入了292例脓毒症患者和31例疑似脓毒症患者的328次菌血症发作。回顾了由革兰氏阴性菌(革兰氏阴性)、革兰氏阳性菌(革兰氏阳性)或真菌引起菌血症患者的病历,并记录了有关PCT和其他炎症标志物的信息。通过受试者操作特征(ROC)曲线计算炎症标志物的诊断性能。
革兰氏阴性、革兰氏阳性和真菌性脓毒症患者的血清PCT水平分别为7.47(四分位间距[IQR]:1.09 - 41.26)ng/mL、0.48(IQR:0.15 - 2.16)ng/mL和0.60(IQR:0.14 - 2.06)ng/mL(<0.001)。ROC分析显示,PCT鉴别革兰氏阴性脓毒症与革兰氏阳性脓毒症的最佳临界值为2.44 ng/mL,敏感性为68.4%,特异性为77.1%。PCT鉴别革兰氏阴性脓毒症与真菌性脓毒症的最佳临界值为3.11 ng/mL,敏感性为63.9%,特异性为93.3%。PCT和其他炎症标志物均无法用于区分革兰氏阳性脓毒症和真菌性脓毒症。
革兰氏阴性脓毒症患者的血清PCT水平显著高于革兰氏阳性或真菌性脓毒症患者。PCT是鉴别革兰氏阴性脓毒症与革兰氏阳性和真菌性脓毒症的潜在敏感生物标志物。