Veauthier Christian, Hasselmann Helge, Gold Stefan M, Paul Friedemann
Interdisciplinary Center for Sleep Medicine, Charité - Universitätsmedizin Berlin, Charitéplatz 1, 10117 Berlin, Germany ; NeuroCure Clinical Research Center, Charité - Universitätsmedizin Berlin, Charitéplatz 1, 10117 Berlin, Germany.
NeuroCure Clinical Research Center, Charité - Universitätsmedizin Berlin, Charitéplatz 1, 10117 Berlin, Germany ; Department of Psychiatry and Psychotherapy, Charité - Universitätsmedizin Berlin, Hindenburgdamm 30, 12203 Berlin, Germany.
EPMA J. 2016 Nov 24;7(1):25. doi: 10.1186/s13167-016-0073-3. eCollection 2016.
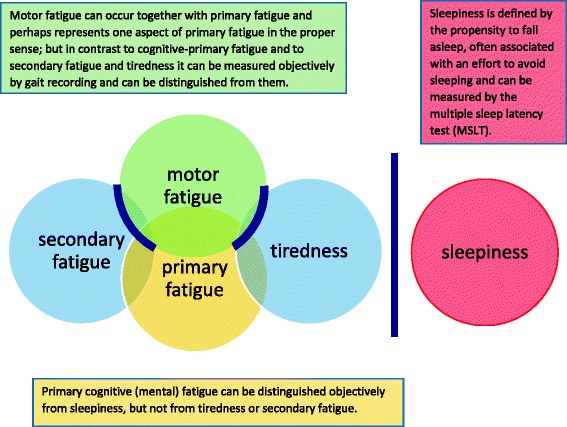
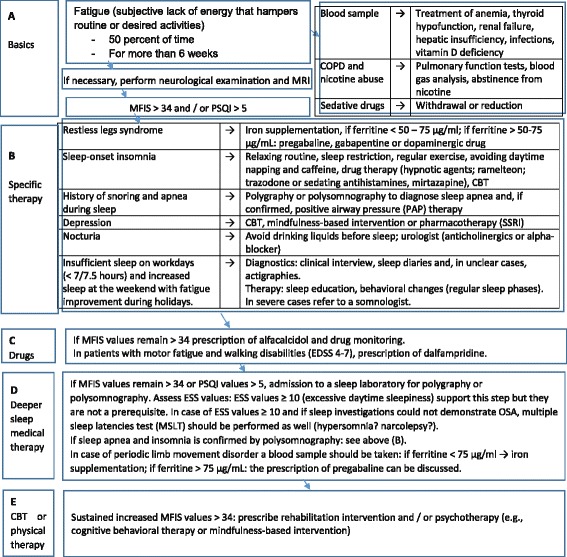
More than 80% of multiple sclerosis (MS) patients suffer from fatigue. Despite this, there are few therapeutic options and evidence-based pharmacological treatments are lacking. The associated societal burden is substantial (MS fatigue is a major reason for part-time employment or early retirement), and at least one out of four MS patients view fatigue as the most burdensome symptom of their disease. The mechanisms underlying MS-related fatigue are poorly understood, and objective criteria for distinguishing and evaluating levels of fatigue and tiredness have not yet been developed. A further complication is that both symptoms may also be unspecific indicators of many other diseases (including depression, sleep disorders, anemia, renal failure, liver diseases, chronic obstructive pulmonary disease, drug side effects, recent MS relapses, infections, nocturia, cancer, thyroid hypofunction, lack of physical exercise). This paper reviews current treatment options of MS-related fatigue in order to establish an individualized therapeutic strategy that factors in existing comorbid disorders. To ensure that such a strategy can also be easily and widely implemented, a comprehensive approach is needed, which ideally takes into account all other possible causes and which is moreover cost efficient. Using a diagnostic interview, depressive disorders, sleep disorders and side effects of the medication should be identified and addressed. All MS patients suffering from fatigue should fill out the Modified Fatigue Impact Scale, Epworth Sleepiness Scale, the Beck Depression Inventory (or a similar depression scale), and the Pittsburgh Sleep Quality Index (or the Insomnia Severity Index). In some patients, polygraphic or polysomnographic investigations should be performed. The treatment of underlying sleep disorders, drug therapy with alfacalcidol or fampridine, exercise therapy, and cognitive behavioral therapy-based interventions may be effective against MS-related fatigue. The objectives of this article are to identify the reasons for fatigue in patients suffering from multiple sclerosis and to introduce individually tailored treatment approaches. Moreover, this paper focuses on current knowledge about MS-related fatigue in relation to brain atrophy and lesions, cognition, disease course, and other findings in an attempt to identify future research directions.
超过80%的多发性硬化症(MS)患者遭受疲劳困扰。尽管如此,治疗选择却很少,且缺乏循证药理学治疗方法。相关的社会负担相当大(MS疲劳是兼职工作或提前退休的主要原因),至少四分之一的MS患者将疲劳视为其疾病最沉重的症状。MS相关疲劳的潜在机制尚不清楚,区分和评估疲劳及疲倦程度的客观标准尚未制定。另一个复杂情况是,这两种症状也可能是许多其他疾病(包括抑郁症、睡眠障碍、贫血、肾衰竭、肝病、慢性阻塞性肺疾病、药物副作用、近期MS复发、感染、夜尿症、癌症、甲状腺功能减退、缺乏体育锻炼)的非特异性指标。本文综述了MS相关疲劳的当前治疗选择,以制定一种考虑到现有合并症的个体化治疗策略。为确保这样的策略也能轻松且广泛地实施,需要一种全面的方法,理想情况下要考虑到所有其他可能的原因,而且还要具有成本效益。通过诊断访谈,应识别并处理抑郁症、睡眠障碍和药物副作用。所有患有疲劳的MS患者都应填写改良疲劳影响量表、爱泼华嗜睡量表、贝克抑郁量表(或类似的抑郁量表)以及匹兹堡睡眠质量指数(或失眠严重程度指数)。在一些患者中,应进行多导睡眠图或全夜睡眠监测检查。治疗潜在的睡眠障碍、使用阿法骨化醇或氨吡啶进行药物治疗、运动疗法以及基于认知行为疗法的干预措施可能对MS相关疲劳有效。本文的目的是确定多发性硬化症患者疲劳的原因,并介绍个体化的治疗方法。此外,本文重点关注与MS相关疲劳有关的脑萎缩和病变、认知、疾病进程及其他发现的当前知识,试图确定未来的研究方向。