DeVries Aaron, Talley Pamela, Sweet Kristin, Kline Susan, Stinchfield Patricia, Tosh Pritish, Danila Richard
Infectious Disease Section, Minneapolis VA Medical Center, Minneapolis, Minnesota, United States of America.
School of Medicine and Public Health, University of Minnesota, Minneapolis, Minnesota, United States of America.
PLoS One. 2016 Dec 1;11(12):e0166797. doi: 10.1371/journal.pone.0166797. eCollection 2016.
In October 2014, the United States began actively monitoring all persons who had traveled from Guinea, Liberia, and Sierra Leone in the previous 21 days. State public health departments were responsible for monitoring all travelers; Minnesota has the largest Liberian population in the United States. The MDH Ebola Clinical Team (ECT) was established to assess travelers with symptoms of concern for Ebola virus disease (EVD), coordinate access to healthcare at appropriate facilities including Ebola Assessment and Treatment Units (EATU), and provide guidance to clinicians.
Minnesota Department of Health (MDH) began receiving traveler information collected by U.S. Customs and Border Control and Centers for Disease Control and Prevention staff on October 21, 2014 via encrypted electronic communication. All travelers returning from Liberia, Sierra Leone, and Guinea during 10/21/14-5/15/15 were monitored by MDH staff in the manner recommended by CDC based on the traveler's risk categorization as "low (but not zero)", "some" and "high" risk. When a traveler reported symptoms or a temperature ≥100.4° F at any time during their 21-day monitoring period, an ECT member would speak to the traveler and perform a clinical assessment by telephone or via video-chat. Based on the assessment the ECT member would recommend 1) continued clinical monitoring while at home with frequent telephone follow-up by the ECT member, 2) outpatient clinical evaluation at an outpatient site agreed upon by all parties, or 3) inpatient clinical evaluation at one of four Minnesota EATUs. ECT members assessed and approved testing for Ebola virus infection at MDH. Traveler data, calls to the ECT and clinical outcomes were logged on a secure server at MDH.
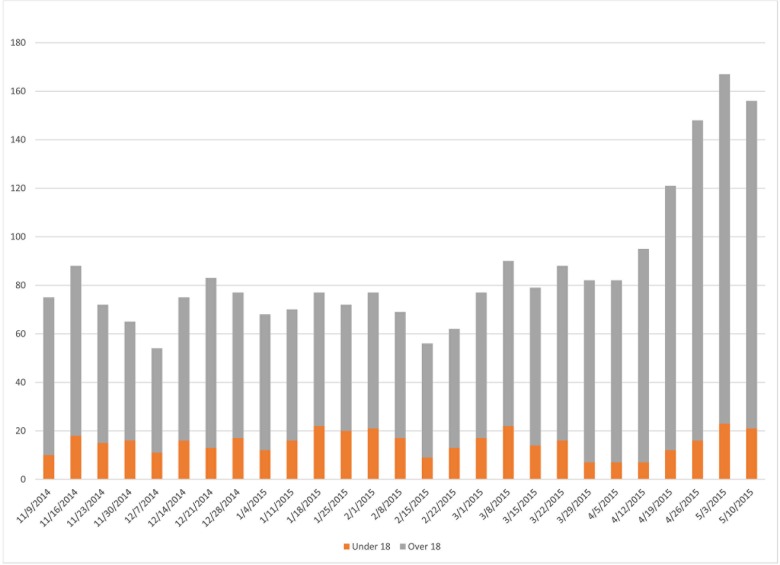
During 10/21/14-5/15/15, a total of 783 travelers were monitored; 729 (93%) traveled from Liberia, 30 (4%) Sierra Leone, and 24 (3%) Guinea. The median number monitored per week was 59 (range 45-143). The median age was 35 years; 136 (17%) were aged <18 years. Thirteen of 256 women of reproductive age (5%) were pregnant. The country of passport issuance was known for 720 of the travelers. The majority of monitored travelers (478 [66%]) used a non-U.S. passport including 442 (61%) Liberian nationals. A total of 772 (99%) travelers were "low (but not zero)" risk; 11 (1%) were "some" risk. Among monitored travelers, 43 (5%) experienced illness symptoms; 29 (67%) had a symptom consistent with EVD. Two were tested for Ebola virus disease and had negative results. Most frequently reported symptoms were fever (20/43, 47%) and abdominal pain (12/43, 28%). During evaluation, 16 (37%) of 43 travelers reported their symptoms began prior to travel; chronic health conditions in 24 travelers including tumors/cancer, pregnancy, and orthopedic conditions were most common. Infectious causes in 19 travelers included upper respiratory infection, malaria, and gastrointestinal infections.
Prior to 2014, no similar active monitoring program for travelers had been performed in Minnesota; assessment and management of symptomatic travelers was a new activity for MDH. Ensuring safe entrance into healthcare was particularly challenging for children, and pregnant women, as well as those without an established connection to healthcare. Unnecessary inpatient evaluations were successfully avoided by close clinical follow-up by phone. Before similar monitoring programs are considered in the future, careful thought must be given to necessary resources and the impact on affected populations, public health, and the healthcare system.
2014年10月,美国开始积极监测此前21天内从几内亚、利比里亚和塞拉利昂旅行归来的所有人。各州公共卫生部门负责监测所有旅行者;明尼苏达州拥有美国最大的利比里亚人口群体。成立了明尼苏达卫生部埃博拉临床团队(ECT),以评估有埃博拉病毒病(EVD)相关症状的旅行者,协调在包括埃博拉评估和治疗单位(EATU)在内的适当医疗机构获得医疗服务,并为临床医生提供指导。
明尼苏达卫生部(MDH)于2014年10月21日开始通过加密电子通信接收美国海关和边境保护局以及疾病控制与预防中心工作人员收集的旅行者信息。2014年10月21日至2015年5月15日期间从利比里亚、塞拉利昂和几内亚返回的所有旅行者,由MDH工作人员按照疾病控制与预防中心推荐的方式,根据旅行者的风险分类为“低(但非零)”、“中等”和“高”风险进行监测。当旅行者在其21天监测期内的任何时间报告出现症状或体温≥100.4°F时,ECT成员会与旅行者通话,并通过电话或视频聊天进行临床评估。根据评估结果,ECT成员会建议:1)在家中继续临床监测,ECT成员通过电话频繁随访;2)在各方商定的门诊地点进行门诊临床评估;3)在明尼苏达州四个EATU之一进行住院临床评估。ECT成员评估并批准在MDH进行埃博拉病毒感染检测。旅行者数据、ECT的通话记录和临床结果记录在MDH的安全服务器上。
在2014年10月21日至2015年5月15日期间,共监测了783名旅行者;729名(93%)来自利比里亚,30名(4%)来自塞拉利昂,24名(3%)来自几内亚。每周监测的中位数人数为59人(范围45 - 143人)。年龄中位数为35岁;136名(17%)年龄<18岁。256名育龄妇女中有13名(5%)怀孕。720名旅行者的护照签发国已知。大多数被监测的旅行者(478名[66%])使用非美国护照,其中包括442名(61%)利比里亚公民。共有772名(99%)旅行者为“低(但非零)”风险;11名(1%)为“中等”风险。在被监测的旅行者中,43名(5%)出现疾病症状;29名(67%)有与EVD一致的症状。两名接受了埃博拉病毒病检测,结果为阴性。最常报告的症状是发热(20/43,47%)和腹痛(12/43,28%)。在评估期间,43名旅行者中有16名(37%)报告他们的症状在旅行前就已开始;24名旅行者的慢性健康状况包括肿瘤/癌症、怀孕和骨科疾病最为常见。19名旅行者的感染原因包括上呼吸道感染、疟疾和胃肠道感染。
2014年之前,明尼苏达州未曾实施过类似的旅行者主动监测项目;对有症状旅行者的评估和管理对MDH来说是一项新活动。确保安全进入医疗机构对儿童、孕妇以及那些与医疗保健没有既定联系的人来说尤其具有挑战性。通过电话密切临床随访成功避免了不必要的住院评估。在未来考虑类似监测项目之前,必须仔细考虑所需资源以及对受影响人群、公共卫生和医疗保健系统的影响。