Khera Rohan, Chan Paul S, Donnino Michael, Girotra Saket
From Division of Cardiology, UT Southwestern Medical Center, Dallas, TX (R.K.); Saint Luke's Mid America Heart and Vascular Institute, Kansas City, and University of Missouri-Kansas City (P.S.C.); Department of Emergency Medicine, Beth Israel Deaconess Medical Center, Boston, MA (M.D.); Division of Pulmonary and Critical Care Medicine, Department of Medicine, Beth Israel Deaconess Medical Center, Boston, MA (M.D.); Division of Cardiovascular Medicine, Department of Internal Medicine, University of Iowa Carver College of Medicine, Iowa City (S.G.).
Circulation. 2016 Dec 20;134(25):2105-2114. doi: 10.1161/CIRCULATIONAHA.116.025459. Epub 2016 Dec 1.
For patients with in-hospital cardiac arrests attributable to nonshockable rhythms, delays in epinephrine administration beyond 5 minutes is associated with worse survival. However, the extent of hospital variation in delayed epinephrine administration and its effect on hospital-level outcomes is unknown.
Within Get With The Guidelines-Resuscitation, we identified 103 932 adult patients (≥18 years) at 548 hospitals with an in-hospital cardiac arrest attributable to a nonshockable rhythm who received at least 1 dose of epinephrine between 2000 and 2014. We constructed 2-level hierarchical regression models to quantify hospital variation in rates of delayed epinephrine administration (>5 minutes) and its association with hospital rates of survival to discharge and survival with functional recovery.
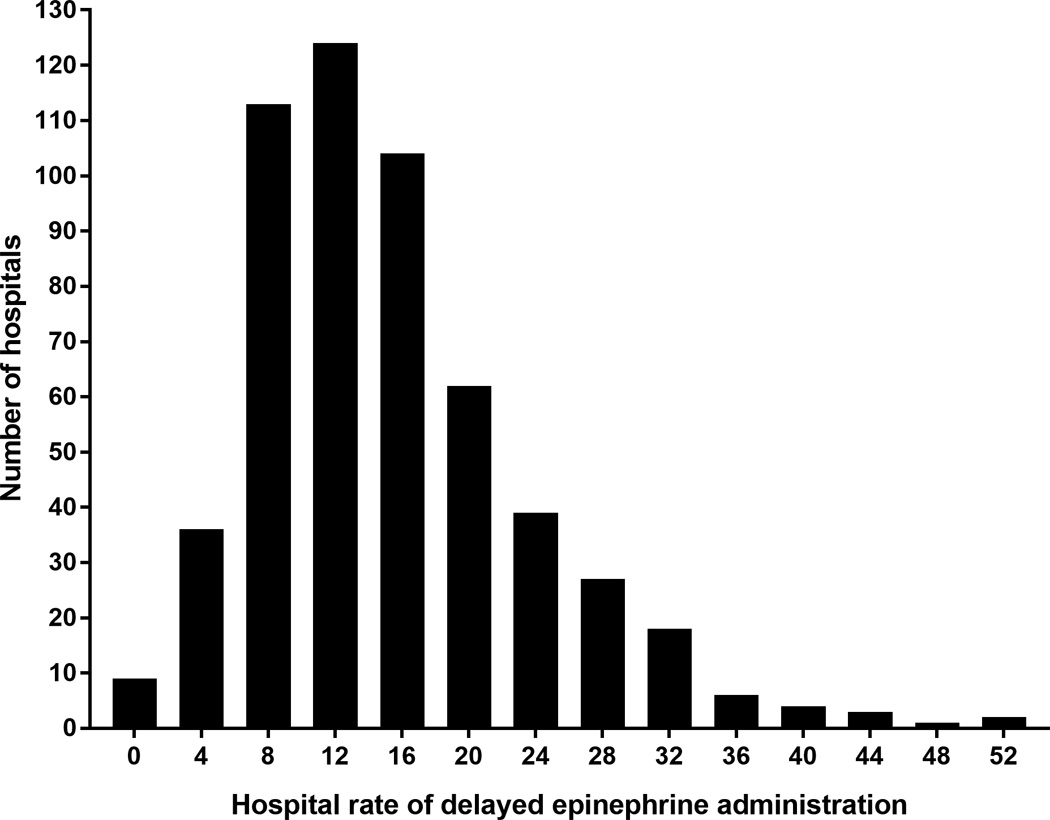
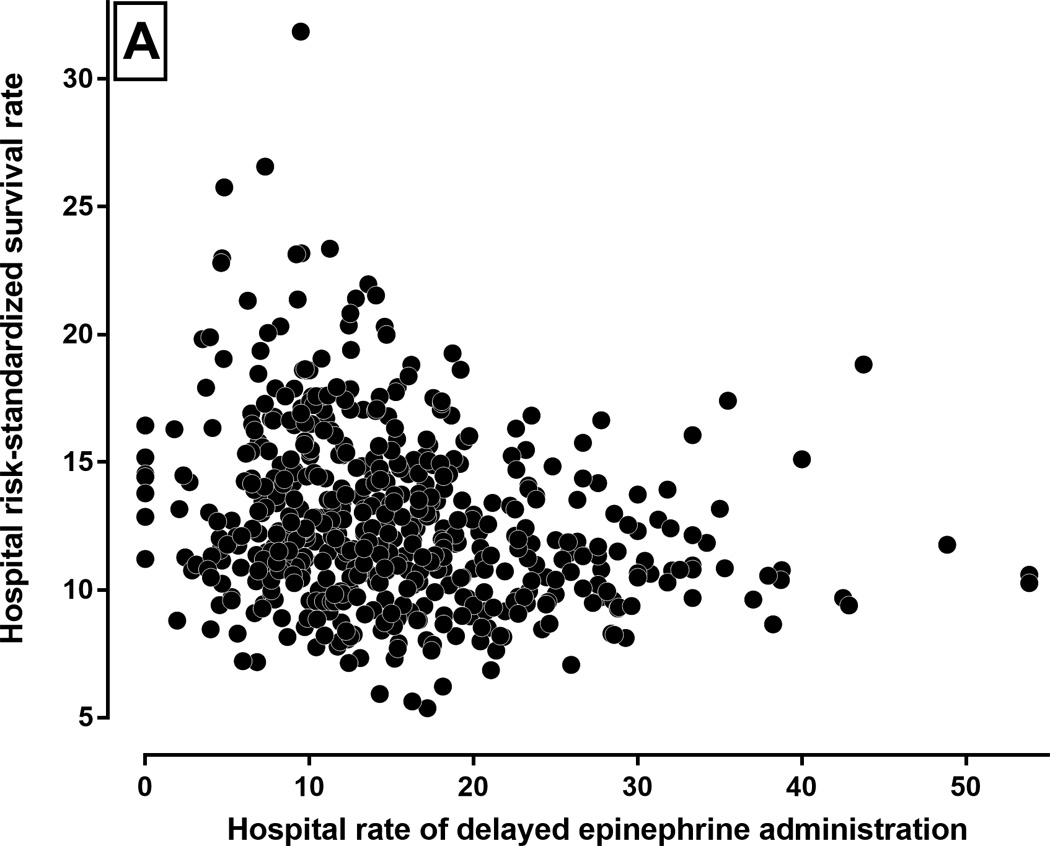
Overall, 13 213 (12.7%) patients had delays to epinephrine, and this rate varied markedly across hospitals (range, 0%-53.8%). The odds of delay in epinephrine administration were 58% higher at 1 randomly selected hospital in comparison with a similar patient at another randomly selected hospital (median odds ratio, 1.58; 95% confidence interval, 1.51-1.64). The median risk-standardized survival rate was 12.0% (range, 5.4%-31.9%), and the risk-standardized survival with functional recovery was 7.4% (range, 0.9%-30.8%). There was an inverse correlation between a hospital's rate of delayed epinephrine administration and its risk-standardized rate of survival to discharge (ρ=-0.22, P<0.0001) and survival with functional recovery (ρ=-0.14, P=0.001). In comparison with a median survival rate of 12.9% (interquartile range, 11.1%-15.4%) at hospitals in the lowest quartile of epinephrine delay, risk-standardized survival was 16% lower at hospitals in the quartile with the highest rate of epinephrine delays (10.8%; interquartile range, 9.7%-12.7%).
Delays in epinephrine administration following in-hospital cardiac arrest are common and variy across hospitals. Hospitals with high rates of delayed epinephrine administration had lower rates of overall survival for in-hospital cardiac arrest attributable to nonshockable rhythm. Further studies are needed to determine whether improving hospital performance on time to epinephrine administration, especially at hospitals with poor performance on this metric, will lead to improved outcomes.
对于因不可电击心律导致的院内心脏骤停患者,肾上腺素给药延迟超过5分钟与较差的生存率相关。然而,医院在肾上腺素给药延迟方面的差异程度及其对医院层面结局的影响尚不清楚。
在“遵循指南-复苏”项目中,我们在548家医院识别出103932例成年患者(≥18岁),这些患者因不可电击心律导致院内心脏骤停,且在2000年至2014年期间接受了至少一剂肾上腺素治疗。我们构建了两级分层回归模型,以量化肾上腺素给药延迟率(>5分钟)的医院差异及其与出院生存率和功能恢复后生存率的医院发生率之间的关联。
总体而言,13213例(12.7%)患者存在肾上腺素给药延迟,且该比率在各医院之间差异显著(范围为0%至53.8%)。与另一家随机选择医院的类似患者相比,在一家随机选择医院中肾上腺素给药延迟的几率高58%(中位数优势比,1.58;95%置信区间,1.51至1.64)。风险标准化生存率中位数为12.0%(范围为5.4%至31.9%),功能恢复后风险标准化生存率为7.4%(范围为0.9%至30.8%)。医院的肾上腺素给药延迟率与其风险标准化出院生存率(ρ=-0.22,P<0.0001)和功能恢复后生存率(ρ=-0.14,P=0.001)之间存在负相关。与肾上腺素延迟率处于最低四分位数的医院的生存率中位数12.9%(四分位间距,11.1%至15.4%)相比,肾上腺素延迟率最高四分位数的医院的风险标准化生存率低16%(10.8%;四分位间距,9.7%至12.7%)。
院内心脏骤停后肾上腺素给药延迟很常见,且各医院之间存在差异。肾上腺素给药延迟率高的医院,因不可电击心律导致的院内心脏骤停的总体生存率较低。需要进一步研究以确定改善医院在肾上腺素给药及时性方面的表现,尤其是在该指标表现较差的医院,是否会导致结局改善。