Pinsky Paul F, Prorok Philip C, Yu Kelly, Kramer Barnett S, Black Amanda, Gohagan John K, Crawford E David, Grubb Robert L, Andriole Gerald L
Division of Cancer Prevention, National Cancer Institute, National Institutes of Health, Bethesda, Maryland.
Division of Cancer Epidemiology and Genetics, National Cancer Institute, National Institutes of Health, Bethesda, Maryland.
Cancer. 2017 Feb 15;123(4):592-599. doi: 10.1002/cncr.30474. Epub 2016 Dec 1.
Two large-scale prostate cancer screening trials using prostate-specific antigen (PSA) have given conflicting results in terms of the efficacy of such screening. One of those trials, the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial, previously reported outcomes with 13 years of follow-up. This study presents updated findings from the PLCO trial.
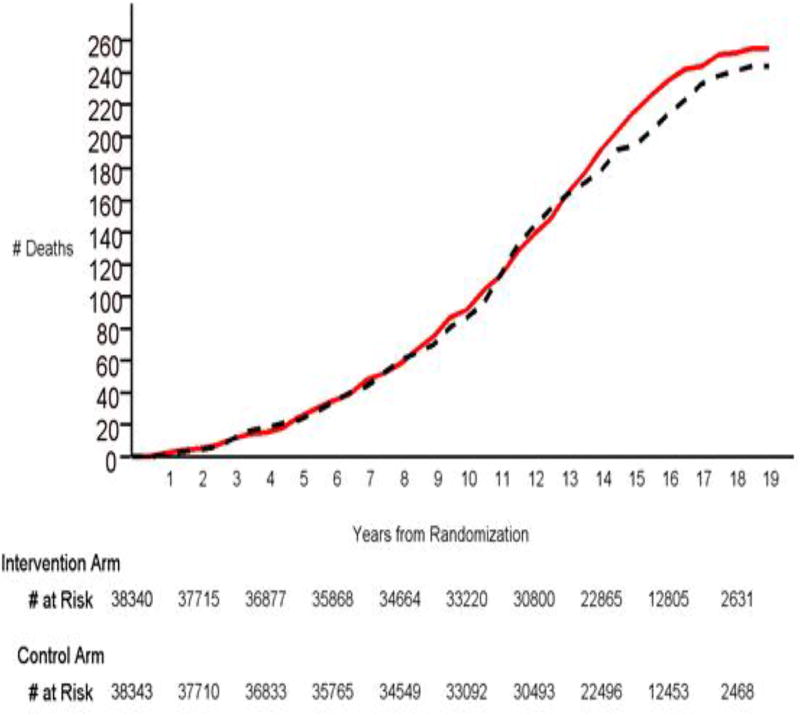
The PLCO trial randomized subjects from 1993 to 2001 to an intervention or control arm. Intervention-arm men received annual PSA tests for 6 years and digital rectal examinations for 4 years. This study used a linkage with the National Death Index to extend mortality follow-up to a maximum of 19 years after randomization.
Men were randomized to the intervention arm (n = 38,340) or the control arm (n = 38,343). The median follow-up time was 14.8 years (25th/75th, 12.7/16.5 years) in the intervention arm and 14.7 years (25th/75th, 12.6/16.4 years) in the control arm. There were 255 deaths from prostate cancer in the intervention arm and 244 deaths from prostate cancer in the control arm; this meant a rate ratio (RR) of 1.04 (95% confidence interval [CI], 0.87-1.24). The RR for all-cause mortality was 0.977 (95% CI, 0.950-1.004). It was estimated that 86% of the men in the control arm and 99% of the men in the intervention arm received any PSA testing during the trial, and the estimated yearly screening-phase PSA testing rates were 46% and 84%, respectively.
Extended follow-up of the PLCO trial over a median of 15 years continues to indicate no reduction in prostate cancer mortality for the intervention arm versus the control arm. Because of the high rate of control-arm PSA testing, this finding can be viewed as showing no benefit of organized screening versus opportunistic screening. Cancer 2017;123:592-599. © 2016 American Cancer Society.
两项使用前列腺特异性抗原(PSA)进行的大规模前列腺癌筛查试验,在这种筛查的疗效方面得出了相互矛盾的结果。其中一项试验,即前列腺、肺、结肠和卵巢(PLCO)癌筛查试验,此前报告了13年随访的结果。本研究展示了PLCO试验的最新发现。
PLCO试验在1993年至2001年将受试者随机分为干预组或对照组。干预组男性接受了6年的年度PSA检测和4年的直肠指检。本研究通过与国家死亡指数联动,将随机分组后的死亡率随访延长至最长19年。
男性被随机分为干预组(n = 38340)或对照组(n = 38343)。干预组的中位随访时间为14.8年(第25/75百分位数,12.7/16.5年),对照组为14.7年(第25/75百分位数,12.6/16.4年)。干预组有255例前列腺癌死亡,对照组有244例前列腺癌死亡;这意味着比率比(RR)为1.04(95%置信区间[CI],0.87 - 1.24)。全因死亡率的RR为0.977(95%CI,0.950 - 1.004)。据估计,对照组中86%的男性和干预组中99%的男性在试验期间接受了任何PSA检测,估计每年筛查阶段的PSA检测率分别为46%和84%。
PLCO试验中位15年的延长随访继续表明,干预组与对照组相比,前列腺癌死亡率没有降低。由于对照组PSA检测率较高,这一发现可被视为表明有组织的筛查与机会性筛查相比没有益处。《癌症》2017年;123:592 - 599。©2016美国癌症协会。