Takahashi Koichi, Wang Feng, Kantarjian Hagop, Doss Denaha, Khanna Kanhav, Thompson Erika, Zhao Li, Patel Keyur, Neelapu Sattva, Gumbs Curtis, Bueso-Ramos Carlos, DiNardo Courtney D, Colla Simona, Ravandi Farhad, Zhang Jianhua, Huang Xuelin, Wu Xifeng, Samaniego Felipe, Garcia-Manero Guillermo, Futreal P Andrew
Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, TX, USA; Department of Genomic Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX, USA; Department of Hematology and Oncology, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
Department of Genomic Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Lancet Oncol. 2017 Jan;18(1):100-111. doi: 10.1016/S1470-2045(16)30626-X. Epub 2016 Dec 3.
Therapy-related myeloid neoplasms are secondary malignancies that are often fatal, but their risk factors are not well understood. Evidence suggests that individuals with clonal haemopoiesis have increased risk of developing haematological malignancies. We aimed to identify whether patients with cancer who have clonal haemopoiesis are at an increased risk of developing therapy-related myeloid neoplasms.
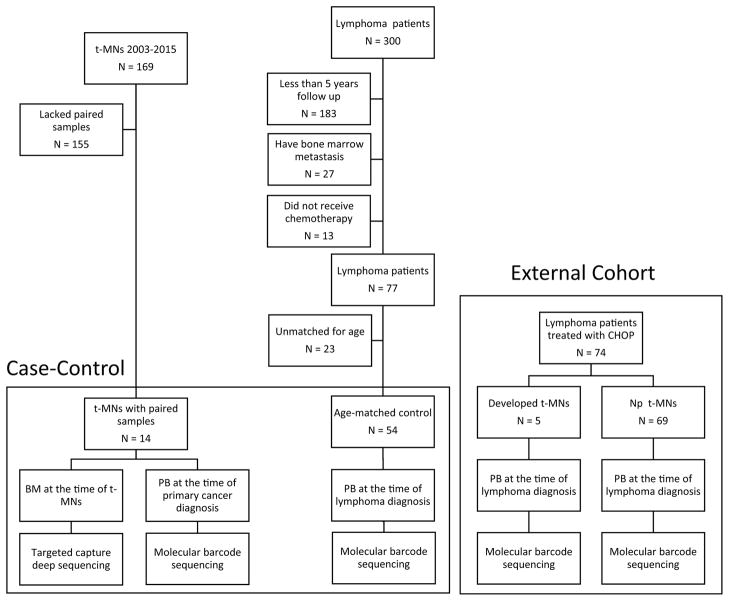
We did this retrospective case-control study to compare the prevalence of clonal haemopoiesis between patients treated for cancer who later developed therapy-related myeloid neoplasms (cases) and patients who did not develop these neoplasms (controls). All patients in both case and control groups were treated at MD Anderson Cancer Center (Houston, TX, USA) from 1997 to 2015. We used the institutional medical database to locate these patients. Patients were included as cases if they were treated for a primary cancer, subsequently developed therapy-related myeloid neoplasms, and had available paired samples of bone marrow from the time of therapy-related myeloid neoplasm diagnosis and peripheral blood from the time of primary cancer diagnosis. Patients were eligible for inclusion as age-matched controls if they were treated for lymphoma, received combination chemotherapy, and did not develop therapy-related myeloid neoplasms after at least 5 years of follow-up. We used molecular barcode sequencing of 32 genes on the pretreatment peripheral blood samples to detect clonal haemopoiesis. For cases, we also used targeted gene sequencing on bone marrow samples and investigated clonal evolution from clonal haemopoiesis to the development of therapy-related myeloid neoplasms. To further clarify the association between clonal haemopoiesis and therapy-related myeloid neoplasm development, we also analysed the prevalence of clonal haemopoiesis in an external cohort of patients with lymphoma who were treated in a randomised trial of front-line chemotherapy with cyclophosphamide, doxorubicin, vincristine, and prednisone, with or without melatonin. This trial was done at MD Anderson Cancer Center between 1999 and 2001 (protocol number 98-009).
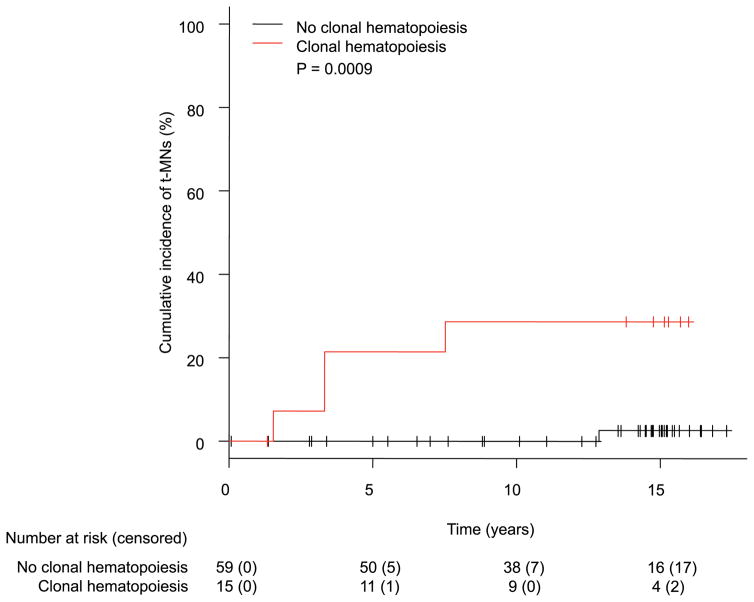
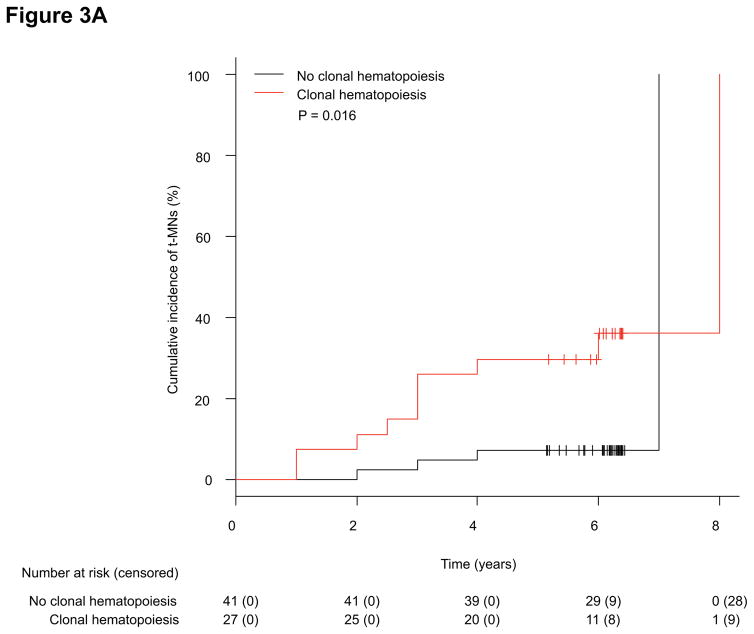
We identified 14 cases and 54 controls. Of the 14 cases, we detected clonal haemopoiesis in the peripheral blood samples of ten (71%) patients. We detected clonal haemopoiesis in 17 (31%) of the 54 controls. The cumulative incidence of therapy-related myeloid neoplasms in both cases and controls at 5 years was significantly higher in patients with clonal haemopoiesis (30%, 95% CI 16-51) than in those without (7%, 2-21; p=0·016). In the external cohort, five (7%) of 74 patients developed therapy-related myeloid neoplasms, of whom four (80%) had clonal haemopoiesis; 11 (16%) of 69 patients who did not develop therapy-related myeloid neoplasms had clonal haemopoiesis. In the external cohort, the cumulative incidence of therapy-related myeloid neoplasms at 10 years was significantly higher in patients with clonal haemopoiesis (29%, 95% CI 8-53) than in those without (0%, 0-0; p=0·0009). In a multivariate Fine and Gray model based on the external cohort, the presence of clonal haemopoiesis significantly increased the risk of therapy-related myeloid neoplasm development (hazard ratio 13·7, 95% CI 1·7-108·7; p=0·013).
Preleukaemic clonal haemopoiesis is common in patients with therapy-related myeloid neoplasms at the time of their primary cancer diagnosis and before they have been exposed to treatment. Our results suggest that clonal haemopoiesis could be used as a predictive marker to identify patients with cancer who are at risk of developing therapy-related myeloid neoplasms. A prospective trial to validate this concept is warranted.
Cancer Prevention Research Institute of Texas, Red and Charline McCombs Institute for the Early Detection and Treatment of Cancer, NIH through MD Anderson Cancer Center Support Grant, and the MD Anderson MDS & AML Moon Shots Program.
治疗相关的髓系肿瘤是继发性恶性肿瘤,通常是致命的,但其危险因素尚未完全明确。有证据表明,具有克隆性造血的个体发生血液系统恶性肿瘤的风险增加。我们旨在确定患有克隆性造血的癌症患者发生治疗相关髓系肿瘤的风险是否增加。
我们进行了这项回顾性病例对照研究,以比较后来发生治疗相关髓系肿瘤的癌症治疗患者(病例组)和未发生这些肿瘤的患者(对照组)之间克隆性造血的患病率。病例组和对照组的所有患者均于1997年至2015年在美国德克萨斯州休斯顿的MD安德森癌症中心接受治疗。我们使用机构医学数据库来查找这些患者。如果患者接受原发性癌症治疗,随后发生治疗相关髓系肿瘤,并且在治疗相关髓系肿瘤诊断时拥有可用的配对骨髓样本以及原发性癌症诊断时的外周血样本,则将其纳入病例组。如果患者接受淋巴瘤治疗、接受联合化疗且在至少5年的随访后未发生治疗相关髓系肿瘤,则符合作为年龄匹配对照组纳入的条件。我们对预处理外周血样本中的32个基因进行分子条形码测序以检测克隆性造血。对于病例组,我们还对骨髓样本进行靶向基因测序,并研究从克隆性造血到治疗相关髓系肿瘤发生的克隆进化。为了进一步阐明克隆性造血与治疗相关髓系肿瘤发生之间的关联,我们还分析了在一项使用环磷酰胺、阿霉素、长春新碱和泼尼松(有或无褪黑素)进行一线化疗的随机试验中接受治疗的淋巴瘤患者外部队列中的克隆性造血患病率。该试验于1999年至2001年在MD安德森癌症中心进行(方案编号98 - 009)。
我们确定了14例病例和54例对照。在14例病例中,我们在10例(71%)患者的外周血样本中检测到克隆性造血。我们在54例对照中的17例(31%)中检测到克隆性造血。克隆性造血患者中病例组和对照组在5年时治疗相关髓系肿瘤的累积发病率(30%,95%CI 16 - 51)显著高于无克隆性造血的患者(7%,2 - 21;p = 0·016)。在外部队列中,74例患者中有5例(7 %)发生治疗相关髓系肿瘤,其中4例(80%)有克隆性造血;69例未发生治疗相关髓系肿瘤的患者中有11例(16%)有克隆性造血。在外部队列中,克隆性造血患者在10年时治疗相关髓系肿瘤的累积发病率(29%,95%CI 8 - 53)显著高于无克隆性造血的患者(0%,0 - 0;p = 0·0009)。在基于外部队列的多变量Fine和Gray模型中,克隆性造血的存在显著增加了治疗相关髓系肿瘤发生的风险(风险比13·7,95%CI 1·7 - 108·7;p = 0·013)。
白血病前期克隆性造血在治疗相关髓系肿瘤患者原发性癌症诊断时且在接受治疗之前很常见。我们的结果表明,克隆性造血可作为一种预测标志物,用于识别有发生治疗相关髓系肿瘤风险的癌症患者。有必要进行一项前瞻性试验来验证这一概念。
德克萨斯州癌症预防研究所、Red和Charline McCombs癌症早期检测与治疗研究所、美国国立卫生研究院通过MD安德森癌症中心支持基金以及MD安德森MDS和AML登月计划。