Das Vidya Nand Ravi, Pandey Ravindra Nath, Siddiqui Niyamat Ali, Chapman Lloyd A C, Kumar Vijay, Pandey Krishna, Matlashewski Greg, Das Pradeep
Rajendra Memorial Research Institute of Medical Sciences (ICMR), Patna, India.
University of Warwick, Coventry, England.
PLoS Negl Trop Dis. 2016 Dec 14;10(12):e0005196. doi: 10.1371/journal.pntd.0005196. eCollection 2016 Dec.
Visceral Leishmaniasis (VL) is a neglected tropical disease that afflicts some of the poorest populations in the world including people living in the Bihar state of India. Due to efforts from local governments, NGOs and international organizations, the number of VL cases has declined in recent years. Despite this progress, the reservoir for transmission remains to be clearly defined since it is unknown what role post kala-azar dermal leishmaniasis (PKDL) and asymptomatic infections play in transmission. This information is vital to establish effective surveillance and monitoring to sustainably eliminate VL.
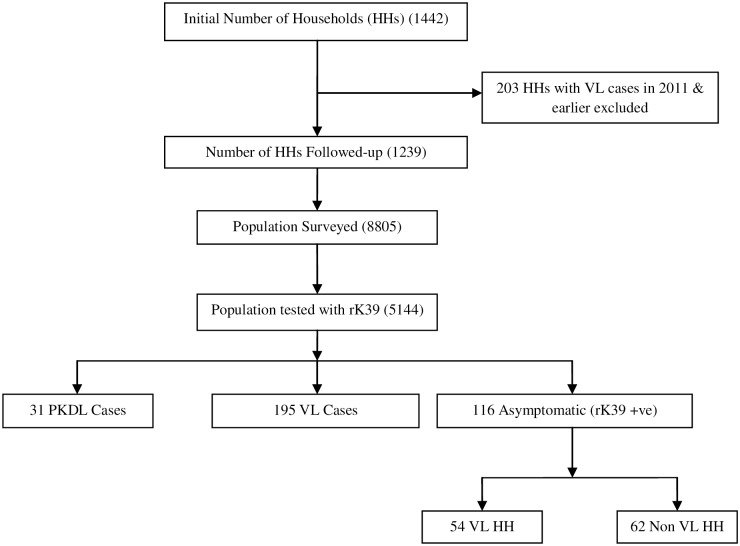
METHODOLOGY/PRINCIPAL FINDINGS: We performed a longitudinal study over a 24-month period to examine VL transmission and seroconversion in households with VL, PKDL and asymptomatic infections in the Saran and Muzaffarpur districts of Bihar. During the initial screening of 5,144 people in 16 highly endemic villages, 195 cases of recently treated VL, 116 healthy rK39 positive cases and 31 PKDL cases were identified. Approximately half of the rK39-positive healthy cases identified during the initial 6-month screening period were from households (HHs) where a VL case had been identified. During the 18-month follow-up period, seroconversion of family members in the HHs with VL cases, PKDL cases, and rK39-positive individuals was similar to control HHs. Therefore, seroconversion was highest in HHs closest to the time of VL disease of a household member and there was no evidence of higher transmission in households with PKDL or healthy rK39-positive HHs. Moreover, within the PKDL HHs, (the initial 31 PKDL cases plus an additional 66 PKDL cases), there were no cases of VL identified during the initial screen or the 18-month follow-up. Notably, 23% of the PKDL cases had no prior history of VL suggesting that infection resulting directly in PKDL is more common than previously estimated.
CONCLUSIONS/SIGNIFICANCE: These observations argue that acute VL cases represent the major reservoir for transmission in these villages and early identification and treatment of VL cases should remain a priority for VL elimination. We were unable to obtain evidence that transmission occurs in HHs with a PKDL case.
内脏利什曼病(VL)是一种被忽视的热带疾病,折磨着世界上一些最贫困的人群,包括生活在印度比哈尔邦的人们。由于地方政府、非政府组织和国际组织的努力,近年来VL病例数量有所下降。尽管取得了这一进展,但传播源仍有待明确界定,因为尚不清楚黑热病后皮肤利什曼病(PKDL)和无症状感染在传播中所起的作用。这些信息对于建立有效的监测以可持续消除VL至关重要。
方法/主要发现:我们在24个月期间进行了一项纵向研究,以调查比哈尔邦萨兰和穆扎法尔布尔地区有VL、PKDL和无症状感染的家庭中的VL传播和血清转化情况。在对16个高度流行村庄的5144人进行初步筛查时,确定了195例近期接受治疗的VL病例、116例健康的rK39阳性病例和31例PKDL病例。在最初6个月的筛查期内确定的rK39阳性健康病例中,约有一半来自已确诊有VL病例的家庭(HHs)。在18个月的随访期内,有VL病例、PKDL病例和rK39阳性个体的家庭中家庭成员的血清转化情况与对照家庭相似。因此,血清转化在最接近家庭成员VL疾病发生时间的家庭中最高,并且没有证据表明PKDL家庭或健康的rK39阳性家庭中有更高的传播率。此外,在PKDL家庭中(最初的31例PKDL病例加上另外66例PKDL病例),在初步筛查或18个月随访期间未发现VL病例。值得注意的是,23%的PKDL病例没有VL病史,这表明直接导致PKDL的感染比以前估计的更为常见。
结论/意义:这些观察结果表明,急性VL病例是这些村庄传播的主要来源,早期识别和治疗VL病例仍应是消除VL的优先事项。我们无法获得证据证明有PKDL病例的家庭中会发生传播。