Etyang Anthony O, Warne Ben, Kapesa Sailoki, Munge Kenneth, Bauni Evasius, Cruickshank J Kennedy, Smeeth Liam, Scott J Anthony G
KEMRI-Wellcome Trust Research Programme, Kilifi, Kenya
London School of Hygiene and Tropical Medicine, London, United Kingdom.
J Am Heart Assoc. 2016 Dec 15;5(12):e004797. doi: 10.1161/JAHA.116.004797.
The clinical and epidemiological implications of using ambulatory blood pressure monitoring (ABPM) for the diagnosis of hypertension have not been studied at a population level in sub-Saharan Africa. We examined the impact of ABPM use among Kenyan adults.
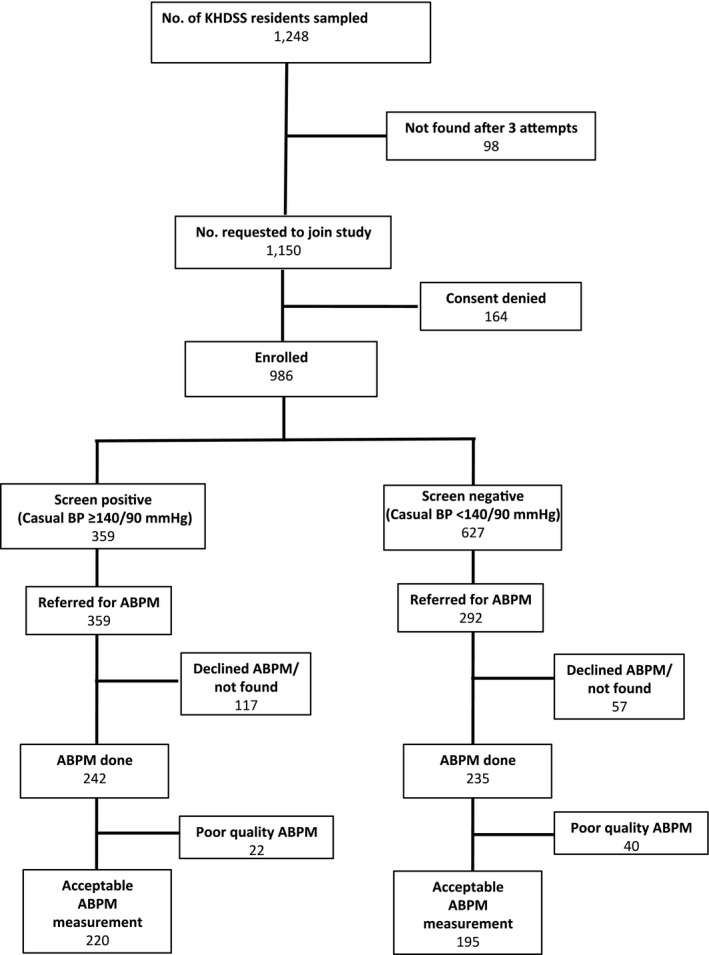
We performed a nested case-control study of diagnostic accuracy. We selected an age-stratified random sample of 1248 adults from the list of residents of the Kilifi Health and Demographic Surveillance System in Kenya. All participants underwent a screening blood pressure (BP) measurement. All those with screening BP ≥140/90 mm Hg and a random subset of those with screening BP <140/90 mm Hg were invited to undergo ABPM. Based on the 2 tests, participants were categorized as sustained hypertensive, masked hypertensive, "white coat" hypertensive, or normotensive. Analyses were weighted by the probability of undergoing ABPM. Screening BP ≥140/90 mm Hg was present in 359 of 986 participants, translating to a crude population prevalence of 23.1% (95% CI 16.5-31.5%). Age standardized prevalence of screening BP ≥140/90 mm Hg was 26.5% (95% CI 19.3-35.6%). On ABPM, 186 of 415 participants were confirmed to be hypertensive, with crude prevalence of 15.6% (95% CI 9.4-23.1%) and age-standardized prevalence of 17.1% (95% CI 11.0-24.4%). Age-standardized prevalence of masked and white coat hypertension were 7.6% (95% CI 2.8-13.7%) and 3.8% (95% CI 1.7-6.1%), respectively. The sensitivity and specificity of screening BP measurements were 80% (95% CI 73-86%) and 84% (95% CI 79-88%), respectively. BP indices and validity measures showed strong age-related trends.
Screening BP measurement significantly overestimated hypertension prevalence while failing to identify ≈50% of true hypertension diagnosed by ABPM. Our findings suggest significant clinical and epidemiological benefits of ABPM use for diagnosing hypertension in Kenyan adults.
在撒哈拉以南非洲地区,尚未在人群层面研究使用动态血压监测(ABPM)诊断高血压的临床和流行病学意义。我们研究了在肯尼亚成年人中使用ABPM的影响。
我们进行了一项关于诊断准确性的巢式病例对照研究。我们从肯尼亚基利菲健康与人口监测系统的居民名单中,按年龄分层随机抽取了1248名成年人。所有参与者都接受了筛查血压(BP)测量。所有筛查血压≥140/90 mmHg的参与者以及部分筛查血压<140/90 mmHg的随机抽取的参与者被邀请接受ABPM。根据这两项检测,参与者被分类为持续性高血压、隐匿性高血压、“白大衣”高血压或血压正常者。分析按接受ABPM的概率进行加权。986名参与者中有359人筛查血压≥140/90 mmHg,粗略的总体患病率为23.1%(95%可信区间16.5 - 31.5%)。年龄标准化的筛查血压≥140/90 mmHg患病率为26.5%(95%可信区间19.3 - 35.6%)。在ABPM检测中,415名参与者中有186人被确诊为高血压,粗略患病率为15.6%(95%可信区间9.4 - 23.1%),年龄标准化患病率为17.1%(95%可信区间11.0 - 24.4%)。隐匿性和“白大衣”高血压的年龄标准化患病率分别为7.6%(95%可信区间2.8 - 13.7%)和3.8%(95%可信区间1.7 - 6.1%)。筛查血压测量的敏感性和特异性分别为80%(95%可信区间73 - 86%)和84%(95%可信区间79 - 88%)。血压指数和有效性指标显示出与年龄密切相关的趋势。
筛查血压测量显著高估了高血压患病率,同时未能识别出约50%通过ABPM确诊的真正高血压患者。我们的研究结果表明,在肯尼亚成年人中使用ABPM诊断高血压具有显著的临床和流行病学益处。