Firima Emmanuel, Retselisitsoe Lefokotsane, Leisa Ikhetheleng, Manthabiseng Molulela, Sematle Mamoronts'ane P, Bane Matumaole, Khomolishoele Makhebe, Gonzalez Lucia, Gupta Ravi, McCrosky Stephen, Lee Tristan, Chammartin Frédérique, Leigh Bailah, Weisser Maja, Amstutz Alain, Burkard Thilo, Labhardt Niklaus Daniel
Division of Clinical Epidemiology, University Hospital Basel, Basel, Switzerland.
Department of Clinical Research, University of Basel, Basel, Switzerland.
EClinicalMedicine. 2023 Aug 30;63:102197. doi: 10.1016/j.eclinm.2023.102197. eCollection 2023 Sep.
WHO introduced the STEPwise approach to surveillance (STEPS) to monitor trends in non-communicable diseases. For arterial hypertension, the STEPS protocol takes the average of the last two out of three standard blood pressure measurements (SBPM). This study assesses the diagnostic accuracy of SBPM, same-day and next-day unattended automated measurement (uABP), with 24 h ambulatory measurement (24 h-ABPM) as reference.
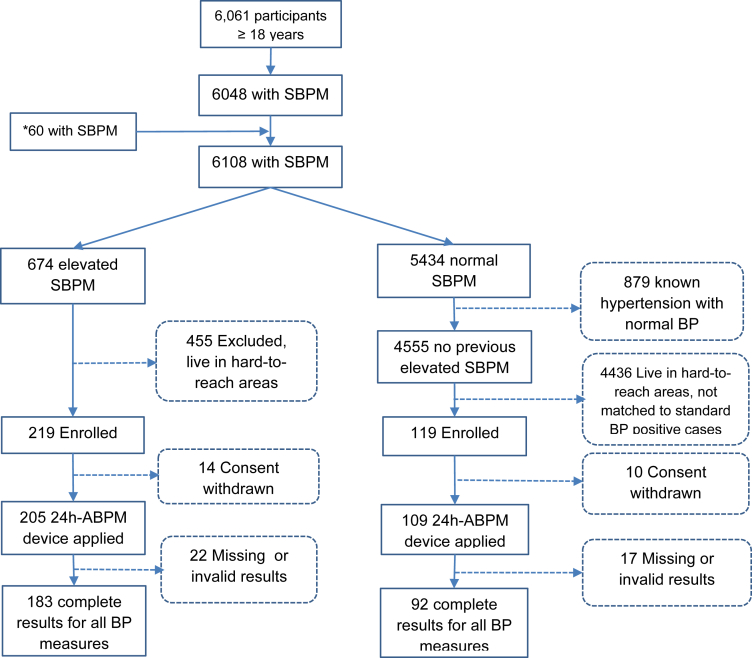
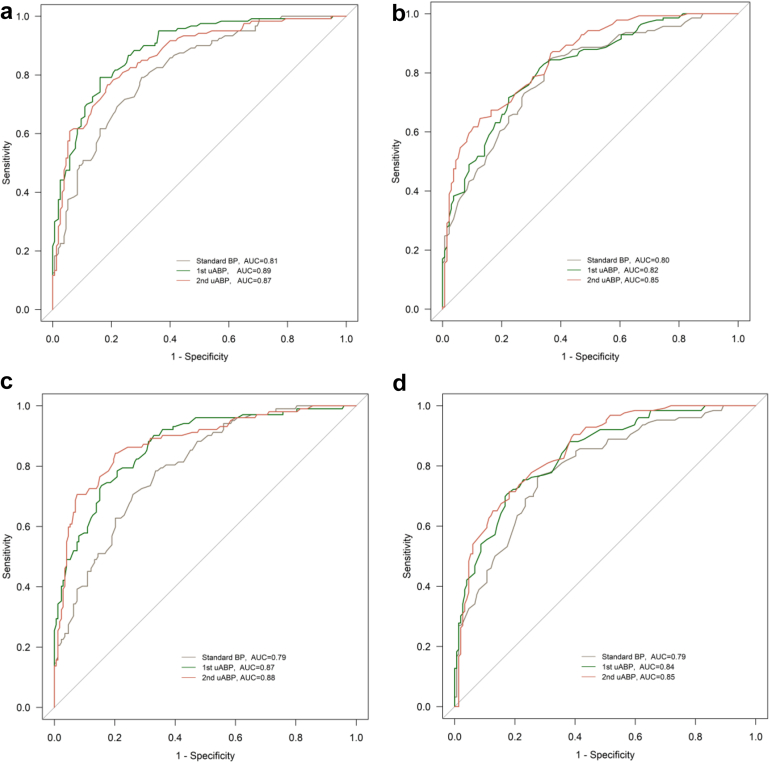
This diagnostic accuracy study was done within a population-based household survey on cardiovascular risk factors in two districts in Northern Lesotho. Adults (aged ≥ 18 years) with elevated SBPM (defined as ≥140/90 mmHg), and 2:1 age- and sex-matched participants with normal SBPM during the survey were recruited. Following SBPM, first uABP readings were obtained on survey day. Afterwards, participants received a 24 h-ABPM device. Second uABP readings were taken 24 h later, after retrieval of the 24 h-ABPM. The main outcome was overall diagnostic accuracy of all screening measurements (SBPM, first uABP, and second uABP), determined using area under the receiver operating characteristic curve (AUROC), with 24 h-ABPM as a reference.
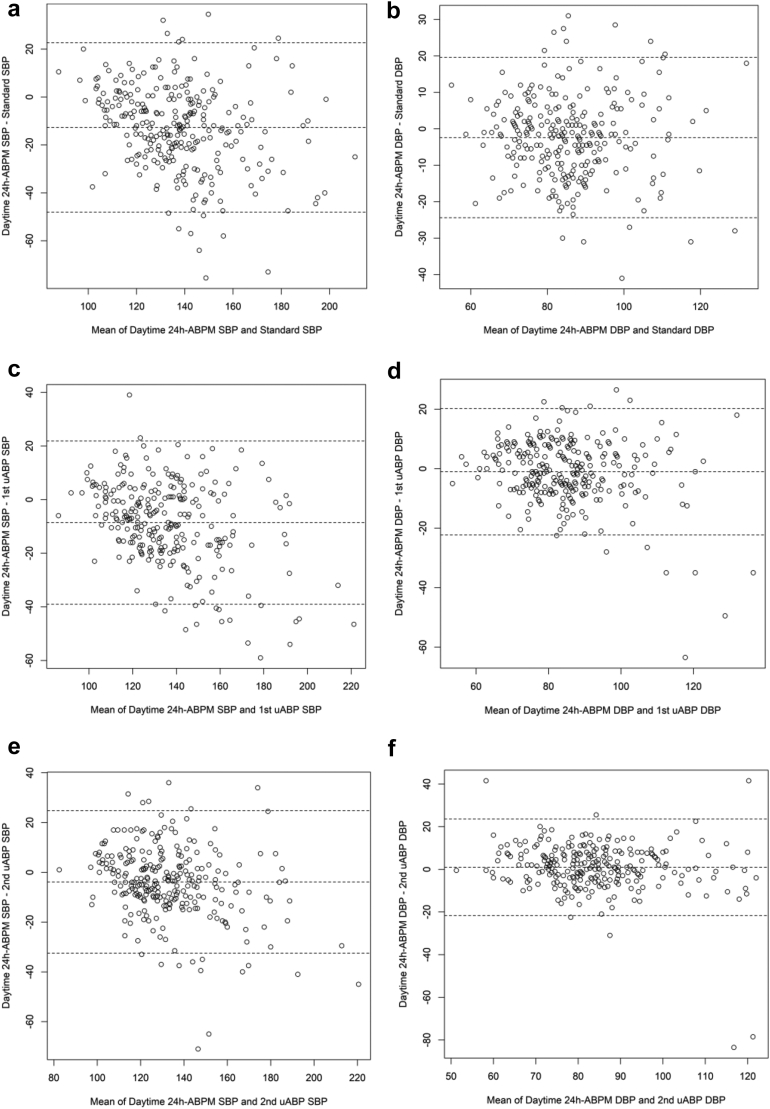
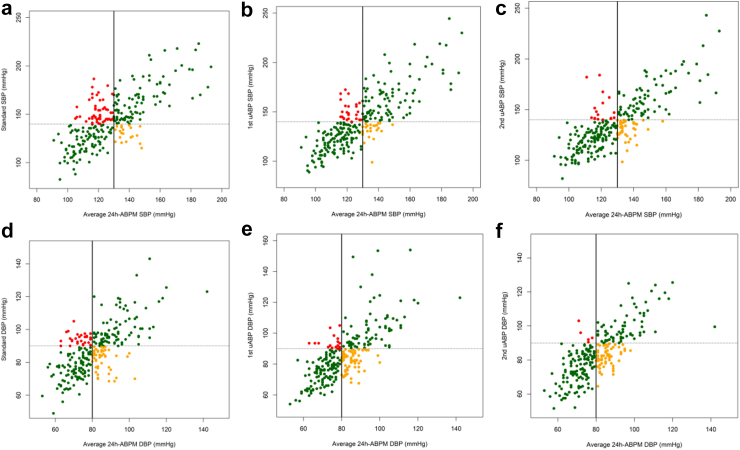
Between November 2, 2021 and August 31, 2022, 275 participants (mean age 58 years (SD: 16 years), 163 (59%) female) were enrolled, 183 of whom had elevated and 92 had normal SBPM. Mean difference between systolic daytime 24 h-ABPM and screening measurements was highest for SBPM (mean difference: -13 mmHg; 95% CI: -14 to -11). Mean difference between diastolic daytime 24 h-ABPM and diastolic SBPM was -2 mmHg (95% CI: -4 to -1), whereas no difference was found for mean diastolic first uABP (mean difference: -1 mmHg; 95% CI: -2.0 to 0.3); and mean diastolic second uABP (mean difference: 1.0 mmHg; 95% CI: -0.4 to 2.3). White coat hypertension was highest with SBPM (55 [20%]), followed by first uABP (27 [9.8%]), and second uABP (18 [6.5%]). Using systolic daytime 24 h-ABPM as a reference, the uABPs had higher AUROC (first uABP: 87% [95% CI: 83-91]; second uABP: 88% [95% CI: 84-92]); SBPM: (79% [95% CI: 74-85]). This difference was significant between first uABP and SBPM ( = 0.0024), and between second uABP and SBPM ( = 0.0017).
uABP had better diagnostic performance than SBPM. Integration of uABP into STEPS protocol should be considered.
Swiss Agency for Development and Cooperation under the ComBaCaL project, and the World Diabetes Foundation.
世界卫生组织引入了逐步监测方法(STEPS)来监测非传染性疾病的趋势。对于动脉高血压,STEPS方案采用三次标准血压测量(SBPM)中最后两次的平均值。本研究以24小时动态血压测量(24 h-ABPM)为参考,评估SBPM、当日和次日无人值守自动测量(uABP)的诊断准确性。
这项诊断准确性研究是在莱索托北部两个地区基于人群的心血管危险因素家庭调查中进行的。招募了SBPM升高(定义为≥140/90 mmHg)的成年人(年龄≥18岁),以及在调查期间SBPM正常的年龄和性别匹配的参与者,比例为2:1。在进行SBPM后,于调查当天获得首次uABP读数。之后,参与者收到一个24 h-ABPM设备。在取回24 h-ABPM后24小时进行第二次uABP读数。主要结果是所有筛查测量(SBPM、首次uABP和第二次uABP)的总体诊断准确性,以24 h-ABPM为参考,使用受试者工作特征曲线下面积(AUROC)来确定。
在2021年11月2日至2022年8月31日期间,共纳入275名参与者(平均年龄58岁(标准差:16岁),163名(59%)为女性),其中183名SBPM升高,92名SBPM正常。收缩期日间24 h-ABPM与筛查测量之间的平均差异在SBPM中最高(平均差异:-13 mmHg;95%置信区间:-14至-11)。舒张期日间24 h-ABPM与舒张期SBPM之间的平均差异为-2 mmHg(95%置信区间:-4至-1),而首次uABP舒张期平均差异未发现差异(平均差异:-1 mmHg;95%置信区间:-2.0至0.3);第二次uABP舒张期平均差异为1.0 mmHg(95%置信区间:-0.4至2.3)。白大衣高血压在SBPM中最高(55例[20%]),其次是首次uABP(27例[9.8%]),第二次uABP(18例[6.5%])。以收缩期日间24 h-ABPM为参考,uABP的AUROC更高(首次uABP:87%[95%置信区间:83-91];第二次uABP:88%[95%置信区间:84-92]);SBPM为(79%[95%置信区间:74-85])。首次uABP与SBPM之间(P = 0.0024)以及第二次uABP与SBPM之间(P = 0.0017)的差异具有统计学意义。
uABP的诊断性能优于SBPM。应考虑将uABP纳入STEPS方案。
瑞士发展与合作署ComBaCaL项目以及世界糖尿病基金会。