Valderhaug Tone G, Aasheim Erlend T, Sandbu Rune, Jakobsen Gunn S, Småstuen Milada C, Hertel Jens K, Hjelmesæth Jøran
Morbid Obesity Centre, Vestfold Hospital Trust, Tønsberg, Norway ; Department of Endocrinology, Akershus University Hospital, Nordbyhagen, Norway ; Division of Medicine and Laboratory Sciences, Institute of Clinical Medicine, University of Oslo, Oslo, Norway ; Tone Gretland Valderhaug, Division of Medicine, Department of Endocrinology, Akershus University Hospital HF, Sykehusveien 25, 1478 Nordbyhagen, Norway.
Department of Health Management and Health Economics, University of Oslo, Oslo, Norway ; Imperial Weight Centre, Imperial College London, London, UK.
BMC Obes. 2016 Dec 7;3:51. doi: 10.1186/s40608-016-0133-1. eCollection 2016.
The King's Obesity Staging Criteria (KOSC) comprises of a four-graded set of health related domains. We aimed to examine whether, according to KOSC, patients undergoing bariatric surgery differed from those opting for conservative treatment.
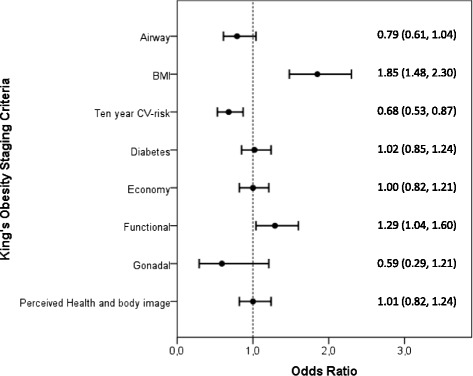
We graded 2142 consecutive patients with morbid obesity attending our centre from 2005-10 into the following KOSC domains: airway/apnoea, body mass index (BMI), cardiovascular risk (CV-risk), diabetes mellitus, economic complications, functional limitations, gonadal dysfunction, and perceived health status/body image. Both patients and physicians agreed upon treatment choice through a shared decision making process.
A total of 1329 (62%) patients opted for lifestyle intervention and 813 (37%) for bariatric surgery as their first treatment choice. The patients treated with bariatric surgery were younger (42 vs. 44 years, < 0.001), had a higher BMI (45.4 vs. 43.8 kg/m, < 0.001) and had a lower ten year estimated CV-risk (9.4 vs. 10.7%, = 0.004) than the lifestyle intervention group. Compared with having BMI < 40 kg/m, BMI ≥ 40 kg/m was associated with 85% increased odds of bariatric surgery (OR 1.85 [95% CI 1.48, 2.30]). Conversely, patients with ≥20% ten year CV-risk, had lower odds of bariatric surgery than patients with <20% CV-risk (0.68 [0.53, 0.87]).
BMI was the strongest KOSC-domain associated with subsequent bariatric surgery after a shared decision making process. Prospective studies are required to assess whether the use of KOSC can help guide patients and clinicians to identify the most appropriate choice of treatment for morbid obesity.
国王肥胖分期标准(KOSC)由一套四级健康相关领域组成。我们旨在研究根据KOSC,接受减肥手术的患者与选择保守治疗的患者是否存在差异。
我们将2005年至2010年在我们中心就诊的2142例连续性病态肥胖患者按照以下KOSC领域进行分级:气道/呼吸暂停、体重指数(BMI)、心血管风险(CV风险)、糖尿病、经济并发症、功能受限、性腺功能障碍以及感知健康状况/身体形象。患者和医生通过共同决策过程就治疗选择达成一致。
共有1329例(62%)患者选择生活方式干预作为首选治疗方法,813例(37%)患者选择减肥手术。接受减肥手术的患者比生活方式干预组更年轻(42岁对44岁,<0.001),BMI更高(45.4对43.8kg/m,<0.001),且十年估计CV风险更低(9.4%对10.7%,=0.004)。与BMI<40kg/m相比,BMI≥40kg/m的患者接受减肥手术的几率增加85%(比值比1.85[95%置信区间1.48,2.30])。相反,十年CV风险≥20%的患者接受减肥手术的几率低于CV风险<20%的患者(0.68[0.53,0.87])。
在共同决策过程后,BMI是与后续减肥手术关联最强的KOSC领域。需要进行前瞻性研究来评估使用KOSC是否有助于指导患者和临床医生为病态肥胖确定最合适的治疗选择。