Baeesa Saleh S, Medrano Belen G, Noriega David C
Division of Neurosurgery, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia.
Spine Unit, Valladolid University Hospital, Royal Academy of Medicine and Surgery, Valladolid, Spain.
Asian Spine J. 2016 Dec;10(6):1100-1105. doi: 10.4184/asj.2016.10.6.1100. Epub 2016 Dec 8.
Retrospective study.
To analyze outcomes of posterior lumbar interbody fusion (PLIF) stand-alone cages.
PLIF for degenerative disk disease using stand-alone cages has lost its popularity owing to implant-related complications and pseudoarthrosis.
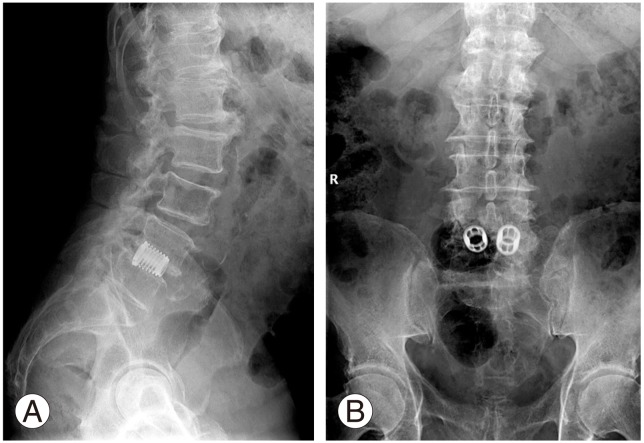
We analyzed the records of 45 patients (18 women, 27 men), operated between January 1994 and December 1996, with a mean follow-up of 18 years 3 months (20 years 3 months-22 years 3 months). Clinical outcomes were measured using visual analogue score (VAS), Oswestry disability index (ODI), Odom's criteria, and radiological measurements of fusion rate, Cobb angle, and implant-related complications conducted at the preoperative evaluation, hospital discharge, 12-month follow-up, and final follow-up.
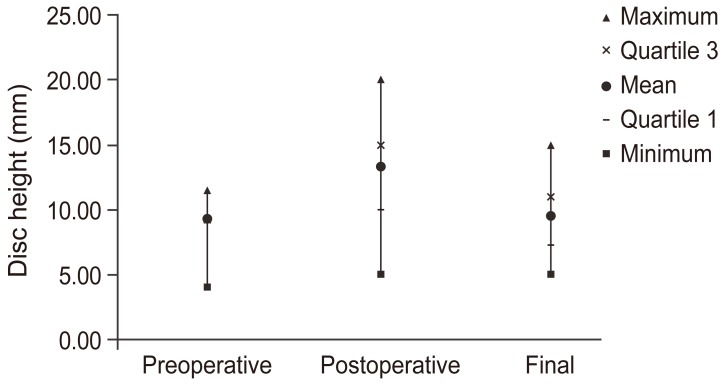
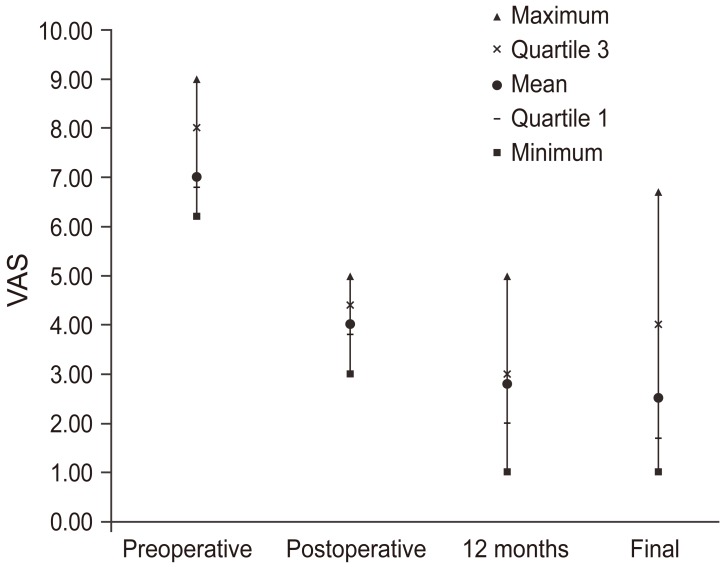
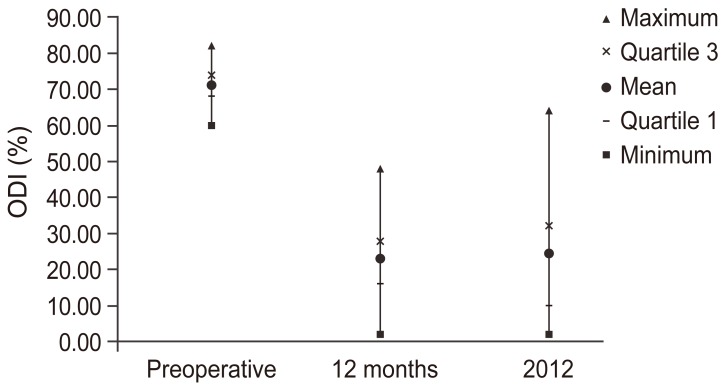
Preoperative mean VAS (back) was 6.9 and VAS (radicular) was 7.2, with mean improvements ( <0.05) of 2.9 and 3.1, respectively, at the final follow-up. Median preoperative ODI was 64.5, with a mean improvement to 34 and 42 at the 12-month and final follow-ups, respectively ( <0.05). Odom's criteria at the 12-month follow-up were excellent in 11.2% patients, good in 57.7%, fair in 31.1%, and poor in none of the patients; at the final follow-up, no patient was classified as excellent, 71.1% as good, 22.2% as fair, and 6.7% as poor ( <0.05). Pseudoarthrosis was observed in five patients (11.1%), of whom, three (6.6%) required re-operation. Preoperative disk height was 9.23 mm, which increased to 13.33 mm in the immediate postoperative evaluation and was maintained at 10.0 mm at the final follow-up ( <0.05). The preoperative mean L1-S1 Cobb angle was 34.7°, which changed to 44.7° in the immediate postoperative evaluation and dropped to 39.7° at the final follow-up ( <0.005).
PLIF stand-alone cages were associated with good clinical outcomes. Although the fusion rate was excellent, maintenance of disk heights and a lordotic alignment were not achieved in the long term.
回顾性研究。
分析后路腰椎椎间融合术(PLIF)单独使用椎间融合器的治疗效果。
由于与植入物相关的并发症和假关节形成,使用单独椎间融合器治疗退行性椎间盘疾病的PLIF已不再受欢迎。
我们分析了1994年1月至1996年12月期间手术的45例患者(18名女性,27名男性)的记录,平均随访时间为18年3个月(20年3个月至22年3个月)。临床结果通过视觉模拟评分(VAS)、Oswestry功能障碍指数(ODI)、奥多姆标准进行评估,并在术前评估、出院时、12个月随访和最终随访时进行融合率、Cobb角和与植入物相关并发症的影像学测量。
术前平均VAS(背部)为6.9,VAS(神经根性)为7.2,在最终随访时分别平均改善了2.9和3.1(<0.05)。术前ODI中位数为64.5,在12个月和最终随访时分别平均改善至34和42(<0.05)。12个月随访时奥多姆标准评估为优秀的患者占11.2%,良好的占57.7%,中等的占31.1%,无差的患者;在最终随访时,无患者被分类为优秀,71.1%为良好,22.2%为中等,6.7%为差(<0.05)。5例患者(11.1%)出现假关节形成,其中3例(6.6%)需要再次手术。术前椎间盘高度为9.23mm,术后即刻评估增加至13.33mm,最终随访时维持在10.0mm(<0.05)。术前L1-S1平均Cobb角为34.7°,术后即刻评估变为44.7°,最终随访时降至39.7°(<0.005)。
PLIF单独使用椎间融合器具有良好的临床效果。尽管融合率良好,但长期来看椎间盘高度和前凸排列未得到维持。